What is the role of transabdominal ultrasound in management of patients with IBD?
What is the role of transabdominal ultrasound in management of patients with IBD?
Kerri Novak, MD
Volume 2 | Issue 7
Runs 2:45
In Crohn’s disease (CD), small bowel imaging techniques are important adjunctive investigations to ileocolonoscopy for various indications, as ileocolonoscopy does not always reliably identify isolated disease, upper gastrointestinal lesions, or extracolonic disease.(1)
Systematic review of imaging modalities
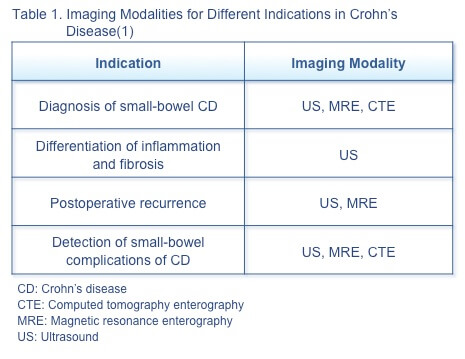
A systematic review of 33 studies of imaging modalities (ultrasound [US], computed tomography enterography [CTE], and magnetic resonance enterography [MRE]) attempted to identify the optimal modality for diagnosis, assessment of postoperative recurrence, and detection of complications in CD (Table 1).(1) Selecting the optimal modality must consider accuracy, safety and tolerability, and factors such as accessibility, availability, and cost. Accuracy is the overriding concern when imaging is a diagnostic procedure or when results are used to guide management. The most important safety considerations are radiation exposure, especially in patients diagnosed at a young age, and adverse events, such as those which may occur with intravenous contrast. Accessibility, availability, and local expertise also affect choice of modality, as delays in obtaining results can affect patient care and delay goal-directed therapy.
Bowel US is inexpensive, well tolerated, requiring no preparation and has potential to be widely available. It is highly sensitive and specific for diagnosis and detection of small-bowel CD activity. It is an ideal option for recurrence detection, but may be limited in its ability to detect stenosis. CTE with oral contrast allows rapid acquisition of small bowel images. Low-radiation techniques can jeopardize accuracy given loss of resolution, although computer modelling techniques can reduce noise associated with low-radiation CTE and improve diagnostic accuracy. CTE has good sensitivity and specificity for detecting stenosis, abscesses, and fistulas.(1)
US in treat to target
Because clinical symptoms do not reliably reflect disease activity, the treat-to-target strategy requires routine objective monitoring to identify disease activity regardless of symptoms in patients with Crohn’s disease.(2) Objective disease monitoring is essential to implementing appropriate therapeutic alterations to achieve mucosal healing and improve outcomes.
This directive, however, is not so simple to implement in clinical practice.(2) The gold standard for objective monitoring, ileocolonoscopy, is not feasible for frequent routine monitoring, as this invasive assessment has associated risks and limits in patient acceptance. Computed tomography (CT) carries concerns about repeatability and cumulative radiation exposure, especially in younger patients. Magnetic resonance imaging (MRI) is an expensive modality with limited access, excluding its routine use.
Transabdominal US has several advantages in monitoring patients with CD as part of the treat-to-target strategy:
- US is safe, noninvasive, well tolerated, repeatable, inexpensive, and available in some centres.(2)
- US can be completed in most patients with CD with few exceptions, such as very high BMI increasing the abdominal wall fat and precluding quality images. This is unlike ileocolonoscopy, which may preclude visualization given stenosis or severe disease.(3)
- US is as effective as CT or MRI in identifying inflammation.(2)
- US has high sensitivity compared with ileocolonoscopy in detecting ileocecal CD, making US a useful initial investigation to map the extent and severity of disease.(2)
- US normalization is a strong predictor of mucosal healing at ileocolonoscopy, possibly reducing the need for invasive monitoring.(3)
- US reliably detects postoperative recurrence and may be a replacement for ileocolonoscopy.(2)
- US effectively detects complications of CD (strictures, fistulas, and abscesses) with a sensitivity as high as 100%.(2)
- US with added contrast can provide additional information for specific uses: a study found contrast-enhanced ultrasound (CEUS) to be comparable to MRE in 105 patients with CD in identifying disease activity.(4) CEUS may be a valuable alternative to MRE for bedside follow-up and contrast may predict early response/ non-response to therapy.(6)
- Bowel US performed in a low-volume centre has comparable diagnostic accuracy for inflammatory bowel changes with that reported in published studies from high-volume centres.(5)
- Bowel US and, in particular, bowel wall thickness can predict increased risk of surgery.(7)
- When applied in clinic during routine follow-up of patients with established Crohn’s disease, there is significant potential to influence clinical decisions, both to adjust or direct therapy and to guide further investigations (8).
Because of these advantages, US can be considered a first-choice imaging modality both for routine surveillance and for evaluation of exacerbations in patients with CD.(2) It will be important to generate data on monitoring with US as part of the treat-to-target strategy.
References
- Greenup AJ, Bressler B, Rosenfeld G. Medical imaging in small bowel Crohn’s disease-computer tomography enterography, magnetic resonance enterography, and ultrasound: “Which one is the best for what?” Inflamm Bowel Dis. 2016;22:1246–61.
- Novak K, Wilson SR. Sonography for surveillance of patients with Crohn disease. J Ultrasound Med. 2012;31:1147–
- Moreno N, Ripolles T, Paredes JM, et al. Usefulness of abdominal ultrasonography in the analysis of endoscopic activity in patients with Crohn’s disease: changes following treatment with immunomodulators and/or anti-TNF antibodies. J Crohns Colitis. 2014;8(9):1079–
- Horje CSHT, Bruijnen R, Roovers L, et al. Contrast enhanced abdominal ultrasound in the assessment of ileal inflammation in Crohn’s disease: a comparison with MR enterography. PLoS One. 2015;10(8):e0136105.
- Sey MS, Gregor J, Chande N, et al. Transcutaneous bowel sonography for inflammatory bowel disease is sensitive and specific when performed in a nonexpert low-volume North American center. J Ultrasound Med. 2013;32:1413–
- Quaia E, Sozzi M, Angileri R et al. Time-intensity curves obtained after microbubble injection can be used to differentiate responders from non-responders among patients with clinically active Crohn disease after 6 weeks of pharmacologic treatment. Radiology. May 18:152461. [Epub ahead of print.]
- Castiglione F, de Sio I, Cozzolino A et al. Bowel wall thickness at abdominal ultrasound and the one-year risk of surgery in patients with Crohn’s disease. Am J Gastroenterol. 2004;99:1977-83.
- Novak K, Tanyingoh D, Petersen F et al. Clinic-based point of care transabdominal ultrasound for monitoring Crohn’s disease: impact on clinical decision making. J Crohns Colitis. 2015:795-801.
Special Edition IBD Dialogue 2016 Volume 02: Treat-to-Target in IBD is made possible by an unrestricted educational grant from…
![]()