What can we learn from the REACT study results?
What can we learn from the REACT study results?
Brian G. Feagan, MD
Volume 2 | Issue 2
Runs 2:22
Overview of REACT*
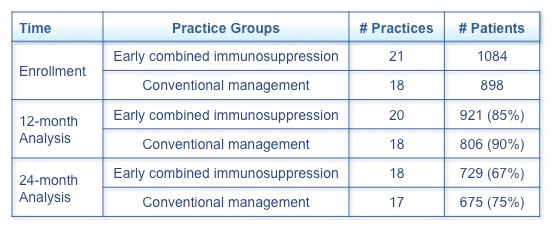
The Randomised Evaluation of an Algorithm for Crohn’s Treatment (REACT), an open-label cluster randomized controlled trial, was performed over a 2-year period in community gastroenterology practices in Belgium and Canada.(1) Practices were randomly assigned to either early combined immunosuppression (n=21) or conventional management (n=18).
The treatment algorithm for early combined immunosuppression mandated initiation of combination immunosuppression with a tumour necrosis factor-α (TNF-α) inhibitor and an antimetabolite in the presence of continuing disease activity after 4 weeks’ (Canada) or 12 weeks’ (Belgium) therapy with a corticosteroid. In REACT, the term early combined immunosuppression refers to the use of combination immunosuppression early in the treatment algorithm rather than early in the disease course, as this term was defined in the top-down vs. step-up trial.(1,2) The proportion of patients in corticosteroid-free remission at 12 months at the practice level was the primary outcome.(1) Important secondary outcomes were the composite rate of major adverse outcomes (surgery, hospitalization admission, or serious disease-related complications) and drug-related adverse effects.
Before the 12-month intention-to-treat analysis of clinical remission, 1 practice withdrew, and after 12 months, 3 practices withdrew for a variety of reasons (Table 1).(1) Relevant demographic factors are disease duration and previous therapies. The mean disease duration was >12 years in the early combined immunosuppression group and >13 years in the conventional management group. Approximately one-third of patients in both groups had previously received treatment with a TNF-α inhibitor, either alone or in combination with an antimetabolite.
Practice-level 12-month remission rates were similar (66.0 ± 14.0% for early combined immunosuppression and 61.0 ± 16.9% for conventional management).(1) All available data were included in the analysis. At 24 months, the composite rate of major adverse outcomes was 27.7% in the early combined immunosuppression practices and 35.1% in the conventional management practices, an absolute difference of 7.3% (hazard ratio [HR] 0.73; 95% confidence interval [CI] 0.62–0.86, P=0.0003). No difference was seen between the treatment groups in drug-related adverse effects, which occurred in approximately 1% of each group. In the early combined immunosuppression group, opportunistic infection was seen in 2 patients and ataxia and confusion in 1 patient.
Table 1. Number of Participating Patients and Practices at Various Time Points
Implications of REACT results
Combination immunosuppressive therapy used early in the treatment algorithm had a nonsignificant benefit upon clinical remission compared with conventional management but a significant reduction in the composite rate of major adverse outcomes.(1) Clinical disease activity correlates poorly with objective measures of inflammation, and clinical remission in the absence of mucosal healing may not decrease the risk of future complications.(3) REACT-II, a proposed follow-up study, would compare outcomes of algorithmic treatment escalation based on ileocolonoscopic findings with escalation based on symptoms alone. Such a study would evaluate the importance of basing treatment decisions on an objective treatment target.
The REACT results suggest both that using symptom-based treatment targets may not prevent bowel damage and that early treatment with highly effective combination immunosuppression may alter the course of Crohn’s disease (CD).(1) Furthermore, the reduction in major adverse outcomes in patients receiving early combined immunosuppression suggests that combination immunosuppression may prevent complications of CD, even in patients with longstanding disease and in those who had previously received biologic therapy. These results extend the findings of the top-down vs. step-up trial, which had previously demonstrated the benefit of early combined immunosuppression very early in the disease course in immunosuppressive-naïve patients.(1,2) Finally, the lack of difference in drug-related adverse effects between the two groups provides evidence of the safety of combination immunosuppression in a community gastroenterology setting.(1)
Treat-to-target and REACT
Evidence has now demonstrated that managing CD with step-up therapy and adjusting treatment based on symptoms is suboptimal.(4) Step-up therapy delays effective treatment in patients with a high risk of disease progression, and basing treatment decisions on symptoms undertreats asymptomatic patients with endoscopic inflammation. The top-down vs. step-up trial, the Study of Biologic and Immunomodulator Naive Patients in Crohn’s Disease (SONIC), and REACT together demonstrate the importance of promptly treating high-risk CD patients with highly effective combination immunosuppression.(1,2,5)
Implementing a treat-to-target strategy may alter the disease course in CD.(4) Such a strategy is based on routinely assessing objective clinical and biological outcomes and refining therapy based on these outcomes to achieve an objective treatment target. However, no definition of a treat-to-target strategy yet exists to allow achievement of treatment goals. In CD, challenges in implementing this strategy include the lack of validated prediction rules allowing individualized risk stratification, the feasibility of serial colonoscopy, and the ability of currently available treatment regimens to achieve mucosal healing.
The optimal treatment target in CD is endoscopic resolution or near-resolution of ulcer lesions.(4) Yet to be determined are a definition of mucosal healing and the benefit of complete vs. partial mucosal healing. In addition, targets may differ in patients with and without structural bowel damage. Furthermore, magnetic resonance enterography or even ultrasound may prove to be an alternative to endoscopy.
Nevertheless, early combined immunosuppression in the context of a treat-to-target strategy holds significant promise for altering the natural history of CD.
*Funding for REACT was provided by AbbVie.
References
- Khanna R, Bressler B, Levesque BG, et al. Early combined immunosuppression for the management of Crohn’s disease (REACT): a cluster randomised controlled trial. Lancet. 2015;386:1825–34.
- D’Haens G, Baert F, van Assche G, et al. Early combined immunosuppression or conventional management in patients with newly diagnosed Crohn’s disease: an open randomised trial. Lancet. 2008;371:660–7.
- Singh S, Loftus EV Jr. Crohn’s disease: REACT to save the gut. Lancet. 2015;386:1800–2.
- Bouguen G, Levesque BG, Feagan BG, et al. Treat to target: a proposed new paradigm for the management of Crohn’s disease. Clin Gastroenterol Hepatol. 2015;13(6):1042–50.
- Colombel JF, Sandborn WJ, Reinisch W, et al. Infliximab, azathioprine, or combination therapy for Crohn’s disease. N Engl J Med. 2010;362:1383–95.
Special Edition IBD Dialogue 2016 Volume 02: Treat-to-Target in IBD is made possible by an unrestricted educational grant from…
![]()