Mental Health and IBD: Supporting the Patient
Mental Health and IBD: Supporting the Patient
January 30, 2023
Introduction: Mental illness in IBD
The objectives of this presentation were to examine the impact of mental health on IBD and discuss ways gastroenterologists can approach communicating about and providing mental health support for their patients.
It is well established that individuals with inflammatory bowel disease (IBD) have an increased risk of mental health concerns. Specifically, depression and clinical anxiety are almost twice as likely for those with IBD compared to those without,1 and an estimated one-third with depression and two-thirds with anxiety go undiagnosed.2,3 Furthermore, the suicide risk is higher in IBD, noting that the rate overall remains low.4,5
The highest risk for comorbid mental illness is around IBD diagnosis5 although a higher risk of depression and anxiety persists throughout the disease course and can be independent of disease activity.5-7 Further, many have onset of mental illness prior to IBD onset.6 The recent pandemic has exacerbated this risk through added challenges such as isolation, financial uncertainty, and health concerns.
Caring for Your IBD Patient
Introducing mental health considerations early in disease care as part of regular assessment is important to improve awareness for both the clinician and patient, validate distress, and facilitate detection of elevated mental health concerns.
It is vital to screen for and promptly address any mental health concerns, as anxiety and depression can negatively impact disease course and treatment outcomes in IBD. Specifically, patients with IBD with comorbid anxiety and/or depression are more likely to experience disease flare, require IBD treatment escalation and corticosteroids, and have higher health care utilization, including increased hospitalizations, emergency room visits, and surgeries.3,8-10
Gastroenterologists are encouraged to talk about mental health early, as they do with bone health, fertility, and other health impacts of IBD. Proactively raising the topic will set the stage for patients to feel safe communicating their mental health experiences. It is recommended that mental health concerns be normalized, validated, and destigmatized. When speaking with patients, it can be helpful to talk about “stress” rather than mental illness as a starting point explaining that stress and distress are common in IBD, and that it is normal to feel overwhelmed at times, as the disease is unpredictable and challenging.
A study on the perspectives of patients and gastroenterologists on psychological factors in IBD found that although 50% of doctors stated that they regularly enquire about these aspects in their clinics, the patients perceived that this was done only 25% of the time.11 A National Institute of Health survey found that among those with IBD and significant psychological distress, only 36% had sought help from a mental health provider in the preceding 12 months.12 Thus, while many gastroenterologists may not feel qualified or comfortable asking about mental health issues, they play an important role in screening and identifying mental health concerns.
Mental Health Screening for Your IBD patients
Gastroenterologists can include a mental health screen as part of their systems review; some simple guidance on how to approach this is provided in Figure 1.
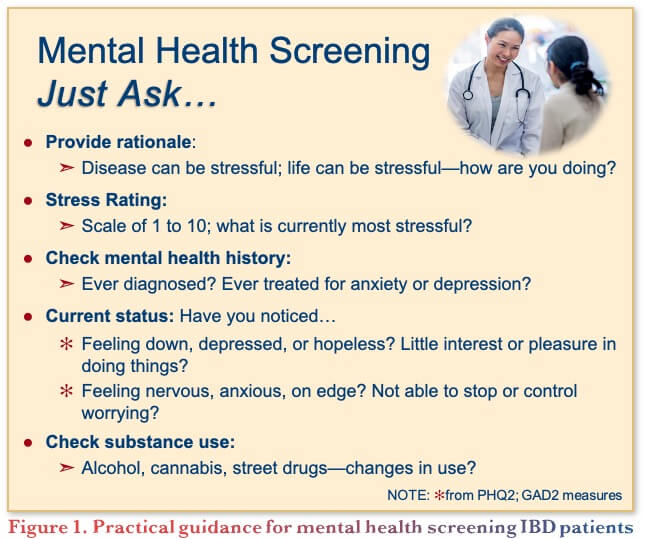
A brief mental health symptom review is also recommended. Anxiety symptoms can be experienced very physically (e.g., increased heart rate, sweating, rapid breathing), in addition to pronounced worry, feeling wound up, and avoidance behavior. Depression is more than just sad mood; symptoms can also include aspects such as loss of interest, difficulty with motivation and finding pleasure, and hopelessness, as well as cognitive (e.g., concentration difficulties) and somatic (e.g., disrupted appetite) symptoms. An important component of identifying the significance of symptoms is to consider their frequency, duration, and degree of interference in day-to-day functioning.
The Mental Health Continuum
Mental health is often described as being on a continuum, which spans severe mental illness (crisis) to thriving and excelling. Clinical treatment aims to shift patients from where they are in the mental illness end of the continuum towards the mentally healthy end of the continuum, which may mean shifting from crisis to struggling and then from struggling to managing, for example. Strengthening resilience can help to prevent stress-related disorders such as anxiety or depression. In addition, in the context of chronic disease, resiliency interventions often focus on managing and thriving despite the illness.
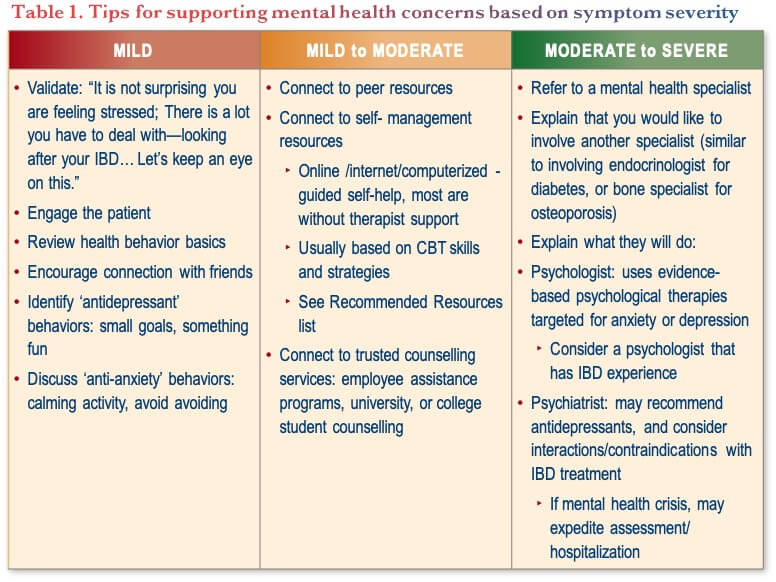
The identification of mild, moderate, or more severe anxiety or depression symptoms can guide potential steps, including patient education, activating support systems and ‘antidepressant behaviors’, the use of online self-guided therapies, and linkage to mental health specialists for targeted therapies. For practical tips on what gastroenterologists can do to support mental health concerns, see Table 1.
Management strategies for Mental Health Concerns in IBD
Psychotherapy
It is helpful for gastroenterologists to have some knowledge of psychological therapies to enhance patient readiness, trust, and willingness to engage. Psychological interventions used with IBD patients include cognitive behavioral therapy (CBT), medical hypnosis, and mindfulness. CBT is a class of therapies with the most robust evidence for depression and anxiety in general, and for IBD patients with comorbid depression and anxiety, with established benefit for mental health concerns and quality of life, and support for positive effects on disease course of IBD as well.13,14 In addition, mindfulness interventions are emerging with promising outcomes for both IBD and comorbid mental health concerns.15,16 Further studies are needed to determine which patients are most likely to benefit from such interventions, and potential mechanisms of action.14
Pharmacotherapies
Antidepressants (e.g., selective serotonin reuptake inhibitors [SSRIs], serotonin and norepinephrine reuptake inhibitors [SNRIs], tricyclic antidepressants [TCAs]) may have a beneficial effect on IBD activity, disease recurrence, IBD-related surgery, quality of life, and treatment compliance, but there is little data directly with IBD patients, and larger randomized studies are needed.17-19
A study of the temporal trends of antidepressant use in IBD found that antidepressants are more likely to be initiated in the year following the IBD diagnosis. However, the majority are receiving treatment for a shorter duration than guidelines recommend, and young adults are more likely to discontinue these medications early.20
Currently, there is insufficient knowledge of whether IBD medication might have a direct effect on depression and anxiety or only works indirectly through the improvement in IBD.14
Conclusions
To summarize, IBD patients are at an increased risk for depression and anxiety compared with the general population. While the risk is particularly high around diagnosis, it can occur at any point in the disease course. Thus, it is recommended that gastroenterologists proactively discuss and routinely monitor mental health status in their patients with IBD. Based on severity of the mental health concerns, they can provide support through patient education, coping strategies, resource guides, and referral to a mental health specialist when moderate to severe. In conclusion, now is the time to ensure mental health is fully incorporated as part of disease management in IBD.
Clinical Case
John—a 19-year-old patient with ileocecal and perianal CD
- On adalimumab EOW monotherapy
- Shows up for clinic follow-up
- Diagnosed at age 14 and was seeing a psychologist while being followed for care in the pediatric GI service
- He has not done pre-clinic bloodwork or FCP
- He describes his ‘overall wellbeing’ as poor and has mild abdominal pain
- Denies EIM or significant diarrhea
- John seems a bit distant and is ‘taking a year off’ from university
- He is back living with his parents and looking for a job
- Denies EtOH use but is using marijuana edibles weekly
- Reports that he is still taking adalimumab but unsure if still covered by parents’ insurance now that he is not in school
- Abdominal exam is unremarkable
- Weight stable
Commentary
With regard to the role of gastroenterologists in screening for mental health concerns:
- The majority screen for mental health, some using the Harvey-Bradshaw Index (HBI) that captures overall wellbeing
- For those that have access to a nurse practitioner, they can also help with the screening process, as patients are more likely to open up to questions around how they are doing, how their work/school is going etc., in a very conversational manner
- Asking questions routinely shows patients their care team is interested in other aspects of health in addition to gut health, and developing a rapport will help patients open up
Case Evolution
- John reports some symptoms of depression and anxiety but denies suicidal thoughts
- He is looking forward to Christmas holidays and returning to school next fall
- You provide him with requisitions for labs and FCP
- John meets with the IBD nurse, who:
- Reviews to assess for any adherence obstacles
- Contacts the patient support program to ensure he has insurance to cover medications
- You book him for a follow-up appointment in 3–4 months
- He returns to clinic in 3 months
- Labs are normal
- FCP is 56 µg/mg
- Minimal IBD-specific symptoms
- Living at home, and not working
- Reports still struggling with mood
- Sleeps a lot and is amotivated
Commentary
- For this case, the majority would provide online resources and send back to primary care for his mental health concerns given his IBD is in remission
- The expert faculty feel a referral to psychiatry is not yet needed.
Case Evolution
- You provide online resources around mental health coping
- You recommend he reduce marijuana intake (due to his amotivation)
- You refer to psychiatry (self-referral if available) if depressive symptoms get worse
- He calls your office to report ongoing depressive symptoms and asks for further recommendations
Commentary
With respect to referral options:
- The ongoing challenge is time constraints and access to mental health services to refer to
- Referral options for psychology or psychiatry may be available through the hospital settings, can work with primary care providers, counselling or psychologist access through work or school settings, etc.
- Some provinces allow self-referral to urgent psychiatric care
- Speaking with their primary care provider directly can facilitate faster referral
- Ultimately, while treating their IBD is important, it does not necessarily mean the psychological aspects are taken care of, so it is important to keep talking about it, regardless of their disease state
Case Evolution
- John returns to clinic
- IBD still clinically and biochemically in remission
- He reports:
- Ongoing depressed mood nearly every day
- 15 lbs weight loss
- Sleeps 12 hours a day
- Fatigued
- Diminished ability to concentrate
Commentary
With regard to prescribing antidepressant therapy:
- The majority of gastroenterologists would ask for help, but some are comfortable prescribing a few options, most likely SSRIs
- Referring to specialists or back to primary care may lead to long wait times, so it may be worthwhile to identify 1–3 antidepressants to become comfortable prescribing
- It is optimal to partner with a psychiatrist to help those patients with significant mental health comorbidities
- Developing a relationship will improve assessment and treatment efficiency, while also being reciprocal in that the gastroenterologist can help with gastrointestinal side effects in the psychiatry setting
- In closing, looking at the big picture, the expert faculty feel it is time to look at incorporating psychological healing as a treatment outcome and measuring progression over time
Recommended resources
General:
- Bounceback – depression bounceback.cmha.ca
- Anxiety Canada – My Anxiety Plan https://maps.anxietycanada.com
IBD-focused:
- Tame Your Gut (Mikocka-Walus Andrews) tameyourgut.com
- IBD Stress Kit (IMAGINE substudy; Furer Graff)
- BOOK: Coping with Crohn’s and Colitis (M. Hunt)
References
-
Bernstein CN, Hitchon CA, Walld R, et al. Increased burden of psychiatric disorders in inflammatory bowel Disease. Inflamm Bowel Dis. 2019;25(2):360-68.
-
Lewis K, Marrie RA, Bernstein CN, et al. The prevalence and risk factors of undiagnosed depression and anxiety disorders among patients with inflammatory bowel disease. Inflamm Bowel Dis. 2019;25(10):1674–80.
-
Sgambato D, Miranda A, Ranaldo R, et al. The role of stress in inflammatory bowel diseases. Curr Pharm Des. 2017;23(27):3997–4002.
-
Malham M, Jakobsen C, Paerregaard A, et al. The incidence of cancer and mortality in paediatric onset inflammatory bowel disease in Denmark and Finland during a 23‐year period: a population‐based study. Aliment Pharmacol Ther. 2019;50(1):1–7.
-
Ludvigsson JF, Olén O, Larsson H, et al. Association between inflammatory bowel disease and psychiatric morbidity and suicide: A Swedish nationwide population-based cohort study with sibling comparisons. J Crohns Colitis. 2021;15(11):1824–36.
-
Walker JR, Ediger JP, Graff LA, et al. The Manitoba IBD cohort study: a population-based study of the prevalence of lifetime and 12-month anxiety and mood disorders. Am J Gastroenterol. 2008;103(8):1989–97.
-
Taft TH, Ballou S, Bedel A, Lincenberg D. Psychological considerations and interventions in inflammatory bowel disease patient care. Gastroenterol Clin North Am. 2017;46(4):847–58.
-
Gracie DJ, Guthrie EA, Hamlin PJ, et al. Bi-directionality of brain-gut interactions in patients with inflammatory bowel disease. 2018;154(6):1635–46.
-
Dubinsky MC, Dotan I, Rubin DT, et al. Burden of comorbid anxiety and depression in patients with inflammatory bowel disease: a systematic literature review. Exp Rev Gastroenterol Hepatol. 2021;15(9):985–
-
Fairbrass KM, Gracie DJ, Ford AC. Relative contribution of disease activity and psychological health to prognosis of inflammatory bowel disease during 6.5 years of longitudinal follow-up. 2022;163:190–203.
-
Marin-Jimenez I, Montoya MG, Panadero A, et al. Management of inflammatory bowel disease: Perspective of doctors and patients – The ENMENTE Project. Inflamm Bowel Dis. 2017;23(9):1492–
-
Greywoode R, Ullman T, Keefer L, et al. National prevalence of psychological distress and use of mental health care in inflammatory bowel disease. Inflamm Bowel Dis. 2022; doi: 10.1093/ibd/izac050. Online ahead of print.
-
Hu S, Chen Y, Chen Y, et al. Depression and anxiety disorders in patients with inflammatory bowel disease. Front Psychiatry. 2021;12:714057.
-
Bisgaard TH, Allin KH, Keefer L, et al. Depression and anxiety in inflammatory bowel disease: epidemiology, mechanisms and treatment. Nat Rev Gastroenterol Hepatol. 2022 (epub ahead of print).
-
Keefer L. Behavioural medicine and gastrointestinal disorders. Nature Rev Gastroenterol Hepatol. 2018;15:378–86.
-
Neilson K, Ftanou M, Monshat K, et al. A controlled study of group mindfulness intervention for individuals living with inflammatory bowel disease. Inflamm Bowel Dis. 2016;22(3):694–701.
-
Mikocka-Walus A, Ford AC, Drossman DA. Antidepressants in inflammatory bowel disease. Nat Rev Gastroenterol Hepatol. 2020;17:184–92.
-
Thorkelson G, Bielefeldt K, Szigethy E. Empirically supported use of psychiatric medications in adolescents and adults with IBD. Inflamm Bowel Dis. 2016;22:1509–22.
-
Goodhand JR, Greig FIS, Koodun Y, et al. Do antidepressants influence the disease course in inflammatory bowel disease? A retrospective case-matched observational study. Inflamm Bowel Dis. 2012;18:1232–9.
-
Jayasooriya N, Blackwell J, Saxena S, et al. Antidepressant medication use in inflammatory bowel disease: a nationally representative population-based study. Aliment Pharmacol Ther. 2022;55(10):1330–41.
Editor-in-Chief
John K. Marshall, MD MSc FRCPC AGAF, Director, Division of Gastroenterology, Professor, Department of Medicine, McMaster University, Hamilton, ON
Contributing Author
Lesley Graff, PhD CPsych, Professor & Head, Department of Clinical Health Psychology, Max Rady College of Medicine, University of Manitoba, Winnipeg, MB
Mentoring in IBD Curriculum Steering Committee
Alain Bitton, MD FRCPC, McGill University, Montreal, QC
Anne M. Griffiths, MC FRCPC, University of Toronto, Toronto, ON
Karen I. Kroeker, MD MSc FRCPC, University of Alberta, Edmonton, AB
Cynthia Seow, MBBS (Hons) MSc FRACP, University of Calgary, Calgary, AB
Jennifer Stretton, ACNP MN BScN, St. Joseph’s Healthcare, Hamilton, ON
IBD Dialogue 2023·Volume 19 is made possible by unrestricted educational grants from…
![]()
![]()
![]()

![]()

![]()
![]()
![]()
Published by Catrile & Associates Ltd., 167 Floyd Avenue, East York, ON M4J 2H9
(c) Catrile & Associates Ltd., 2023. All rights reserved. None of the contents may be reproduced in any form without prior written permission from the publisher. The opinions expressed in this paper are those of the authors and do not necessarily reflect the opinions or recommendations of the sponsors, the grantor, or the publisher.