Cancer and IBD: Does My Treatment Cause Cancer?
Cancer and IBD: Does My Treatment Cause Cancer?
April 13, 2021
Introduction
Patients with inflammatory bowel disease (IBD) are at increased risk for malignancy, likely due to innate immune dysfunction, ongoing inflammation, and immunosuppressive therapies used for treatment.
This review provides a summary of the epidemiology of malignancy in IBD; the risks of malignancy associated with IBD therapies; a discussion of what to do in the case of recurrence of malignancy; some tips on how to communicate risk of malignancy to patients; and preventive strategies for malignancy in IBD.
Epidemiology of malignancy in IBD
Overall, individuals with IBD are at increased risk of malignancy compared to the general population. Illustrative data include a 2016 study from a Dutch cohort of 1,157 patients with Crohn’s disease (CD) and 1,644 patients with ulcerative colitis (UC), diagnosed between 1991 and 2011.(1) In this analysis, the authors reported a total of 79 primary cancers among 73 CD patients. This translated into modestly increased overall cancer risk for CD compared to the general Dutch population (standardized incidence ratio [SIR] 1.28; 95% confidence interval [CI] 1.01–1.60). Those subgroups who were found to be at significantly increased risk were: males (SIR 1.41), those older than 40 years of age at CD diagnosis (SIR 1.36), those with ileal localization at CD diagnosis (SIR 1.38) and those in the first decade after CD diagnosis (SIR 1.54).
The individual malignancies with increased risk in the CD cohort compared to the general population were hematologic cancers (SIR 2.41; 95% CI 1.04–4.76) and skin cancer (SIR 1.55; 95% CI 1.06–2.19), particularly squamous cell carcinoma (SIR 3.83; 95% CI 1.83–7.04). There was also one malignancy with a lower risk among patients with CD: breast cancer (SIR 0.11; 95% CI 0.00–0.64).
In the total UC population, 172 primary cancers were observed in 158 UC patients. Overall cancer risk was similar to the background population (SIR 1.03; 95% CI 0.88–1.20). The only factor identified as being significantly associated with increased overall malignancy risk was being in the second decade after UC diagnosis (SIR 1.39); 95% CI 1.10–1.73).
There were no individual malignancies identified as being higher or lower risk among subjects with UC compared to the general population.
With respect to longitudinal trends, research indicates that rates of gastrointestinal malignancy have declined over time among patients with IBD, without an increase in extraintestinal malignancies.(2)
Risks of Malignancy Associated with Therapies
The malignancy risks associated with various IBD therapies are summarized in the Table.(3-6) Most relevant are increased risks of lymphoma and non-melanoma skin cancer (NMSC), each of which has a differing risk profile for the various agents used for the treatment of IBD. There are particular considerations to keep in mind with thiopurines, in monotherapy or in combination with anti-TNF agents. Notably, the newer biologic agents, vedolizumab and ustekinumab, have not been associated with increased risks of either lymphoma or NMSC.(5,6)

Lymphoma
With respect to lymphoma, a systematic review of published evidence showed that the vast majority of cases (84%) of lymphoma among people with IBD are of non-Hodgkin’s lymphoma (NHL) type; a large proportion (22 to 75% across the studies) were primary intestinal lymphoma; and a large proportion were Epstein-Barr virus (EBV)-positive (45 to 75%).(7)
Both thiopurines and anti-TNF therapies have been associated with increased risk of lymphoma among IBD patients. In a National French database study of 189,298 adult IBD patients followed for a mean of 6.7 years, the incidence rate (IR) of lymphoma among people unexposed to either thiopurine or anti-TNF therapy was 0.26 per 1000 patient-years (95% CI 0.23–0.29). There was an increase in risk associated with anti-TNF monotherapy (IR 0.41, 95% CI 0.27–0.55), thiopurine monotherapy (IR 0.55, 95% CI 0.41–0.67) and the combination of thiopurine and anti-TNF (IR 0.95, 95% CI 0.45–1.45).(8) After adjusting for confounders, the hazard ratios (HRs) for lymphoma compared to unexposed patients were: 2.60 for thiopurine monotherapy (95% CI 1.96–3.44); 2.41 for anti-TNF monotherapy (95% CI 1.60–3.64); and 6.11 for the combination (95% CI 3.46–10.80).(8)
Importantly, when thiopurine therapy is discontinued, the lymphoma risk drops significantly. A study from a French cohort (N=19,486 patients with IBD) reported that the incidence rates of lymphoproliferative disorders were 0.90 per 1000 (95% CI 0.50–1.49) patient-years in those receiving thiopurines, 0.20/1000 (95% CI 0.02–0.72) patient-years in those who had discontinued, and 0.26/1000 (95% CI 0.10–0.57) patient-years in those who had never received thiopurines (p=0.0054).(9)
A modelling study published in 2016 sought to determine whether or not it was prudent to discontinue thiopurine therapy for CD patients in sustained clinical remission, with respect to improving safety, including malignancy risk.(10) The study showed that thiopurines are protective up to a certain age, but then are associated with increased risk of lymphoma (and colorectal cancer).(10) The study determined that threshold at which withdrawing thiopurine therapy was associated with optimal overall survival was 40.6 years for men, and 45.7 years for women—among those without extensive colitis. For those with extensive colitis, however, it was recommended that thiopurine therapy be continued indefinitely.(10)
One type of lymphoma that is of particular concern in the setting of IBD is hepatosplenic T-cell lymphoma (HTCL). This is a very rare, aggressive extranodal form of NHL, with a mean time from diagnosis to death of less than 16 months.(11-13) HTCL does occur de-novo in general population (only 10% of cases are related to IBD treatment), but increased risk has been identified in IBD in the context of combination therapy with a thiopurine and an anti-TNF agent (but not with anti-TNF therapy alone).(11-13) Those individuals who are at highest risk for HTCL among patients with IBD are young males.(11-13)
Non-melanoma skin cancer
Thiopurines, anti-TNF agents and methotrexate have all been associated with increased risks of NMSC in the context of IBD.(14) A retrospective case-control study using a US administrative database matched each of 387 CD patients and 355 UC patients with NMSC to four IBD patients without NMSC.(14) This analysis showed that persistent use (>one year duration) of thiopurines was associated with a greater than 4-fold risk of NMSC in both CD and UC.(14) Anti-TNF agents were also associated with increased risk of NMSC in CD (odds ratios [OR] 2.18, 95% CI 1.07–4.46). There was also a non-significant trend towards increased risk of NMSC with methotrexate among patients with CD (OR 2.69, 95% CI 0.63–11.56).(14).
The proposed mechanisms of increased NMSC risk associated with thiopurines is photosensitization of skin to UVA light. This enhances sunlight-induced chronic oxidative stress and increases the levels of oxidative DNA skin lesions.(15,16)
To date, there have been no data demonstrating an increased risk of NMSC in RCTs for vedolizumab or ustekinumab vs. placebo.(5,6) Any rare cases of NMSC in these programs had prior exposure to azathioprine and/or an anti-TNF agent. Ustekinumab has a much larger body of evidence in dermatology, where it has been used to treat psoriasis for many years. In the PSOLAR registry of biologics and DMARDs for psoriasis (n=12,090, 48,870 patient-years), the incidence of on-treatment NMSC for ustekinumab was 0.19 per 100 patient-years, which was significantly lower than the rates observed with anti-TNF biologics (incidence 0.43/100 patient-years).
Tofacitinib, the first oral JAK inhibitor to be approved for use in IBD, has also been linked to a possible increased risk of NMSC. This was first identified in the rheumatology field, where tofacitinib has been used for the treatment of rheumatoid and psoriatic arthritis for many years.(17) In that setting, the incidence of NMSC has been reported to be 55 per 100 patient-years, with lower doses (5 mg b.i.d.) associated with lower NMSC risk compared to higher doses (10 mg b.i.d.).(17) Data from the UC development program of tofacitinib have shown similar estimates.(18)
Melanoma
IBD is associated with an overall increased risk of melanoma. In a large meta-analysis involving a total of 172,837 patients from 12 studies, the relative risk (RR) for melanoma was 1.37 (95% CI 1.10–1.70) for IBD vs. the general population. The association was somewhat more pronounced for CD (RR 1.80; 95% CI 1.17–2.75). Similar results were seen in a retrospective US database study involving 108,579 patients with IBD, each matched to 4 individuals without IBD.(4)
With respect to the impact of IBD therapies, a nested case-control analysis from within the same US database showed that anti-TNF therapy was associated with a significant increase in risk for melanoma in IBD overall (OR 1.88, 95% CI 1.08–3.29) and in CD (OR 1.94, 95% CI 1.03–3.68), but the result for UC was not statistically significant (OR 1.73, 95% CI 0.53–5.63).(4) Neither thiopurines nor 5-ASA therapies were associated with any significant impact on melanoma rates.(4)
Recurrence of Malignancy
Recurrence risk for malignancy among patients with IBD is based on the individual type of cancer. Data to date are reassuring, albeit limited, with regard to the impact of various IBD therapies on recurrence.(20) A meta-analysis of studies investigating the impact of immunosuppressive therapies across indications (eight studies in IBD, nine in rheumatoid arthritis and one in psoriasis) included a total of 11,707 subjects with a prior diagnosis of cancer with a total of 31,258 patient-years of follow up. In that cohort, there was no significant difference in recurrence rates between those receiving anti-TNF therapies (recurrence rate for cancer: 33.8 per 1000 patient-years), those receiving a conventional immunomodulator (36.2 per 1000 patient-years) or those with no immunosuppression (37.5 per 1000 patient-years).(20) The recurrence rate was numerically higher for combination immunomodulator therapy (54.5 per 1000 patient-years), but the difference vs. no immunomodulator therapy was not statistically significant. Although these data are encouraging, the meta-analysis did have limitations, including concerns surrounding selection bias and lack of data on early re-initiation of therapy.
In the context of IBD, investigators working with data from the CESAME prospective observational cohort identified 405 patients with cancer diagnosed previous to study entry.(21) They reported that the incidence of cancer was significantly higher among those with previous cancer at entry than among those without prior history (HR 1.9, 95% CI 1.2–3.0, p=0.003). With respect to IBD therapy, no statistically significant association was found between immunosuppressant exposure and the risk of new or recurrent cancer, although the incidence was numerically higher for those with immunosuppressant use.
A more recent retrospective analysis evaluated the incidence of new or recurrent cancer among IBD patients with current or prior malignancy.(22) Patients in this retrospective analysis from a healthcare system in Boston were stratified as having had anti-TNF therapy (n=184), vedolizumab (n=96) or no immunosuppressive therapy (n=183) after the index cancer diagnosis. For the primary study outcome of new primary cancer or recurrent cancer, there was no difference in risk associated with either vedolizumab or anti-TNF therapy compared to no immunosuppression (after adjustment for age, IBD subtype, smoking, antimetabolite exposure, cancer category, cancer stage, and time to biologic). This was true regardless of whether or not NMSC was included in the analysis.
Practical Management of IBD Therapy in the Setting of Malignancy—A Case Example
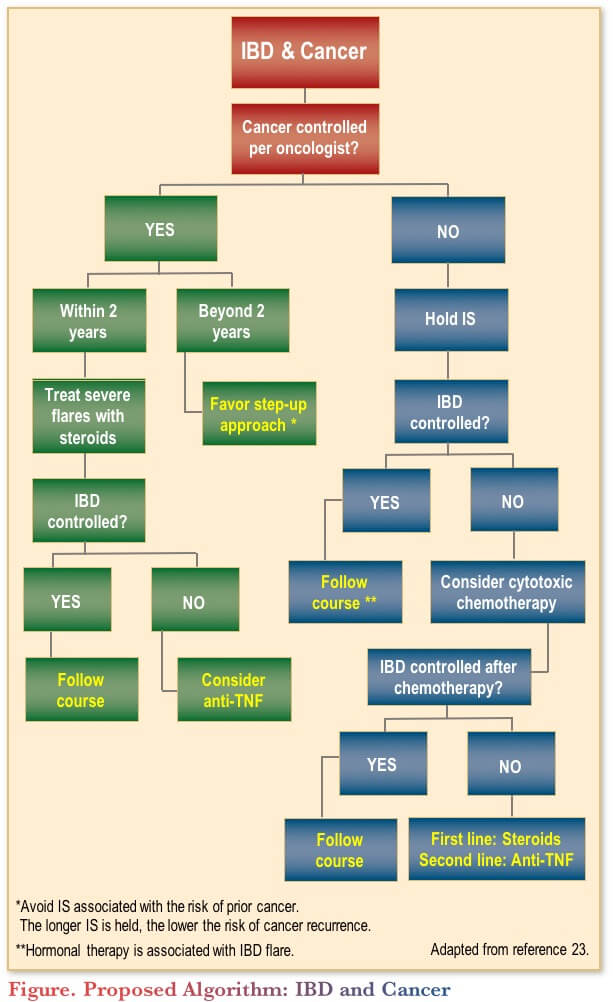
A 2013 paper written by a group of gastroenterologists included a practical algorithm to help guide the selection of therapy for IBD patients with active cancer (Figure). While the paper predates the availability of vedolizumab, ustekinumab and tofacitinib, it is still a useful guide to help clinicians with therapeutic decision-making in the setting of IBD and cancer.
Case example
To illustrate how this algorithm might be used, consider the following case. Sarah is a 48-year-old woman with CD: ileocolonic (predominantly rectal and ileal), with perianal phenotype. She has a history of ileal resection, after which she was maintained on adalimumab and achieved endoscopic remission.
She was subsequently diagnosed with breast cancer, with three locally invasive ductal tumours (small in size). Following lumpectomy, there were positive margins, but negative lymph nodes. She then received chemotherapy (adriamycin and paclitaxel) and underwent bilateral mastectomy. During the chemotherapy, her adalimumab was held, and she was maintained on budesonide, with continued remission of her CD.
After chemotherapy, CD symptoms and fecal calprotectin began to increase; vedolizumab was then initiated. One year later, a colonoscopy showed a Rutgeert’s score of I0, and there was no residual tumor as of three years. She was told by her oncologist that she was in remission.
Subsequently, she presented with increased bowel movement frequency, and new perirectal pressure and drainage. Colonoscopy showed a Rutgeert’s score of I2, with active perianal fistula. Surgery was performed to drain the abscess, and a seton was placed.
The questions one might ask at this point are:
- What IBD therapy would be most appropriate now?
- Would there be an increased risk of cancer recurrence concern with an anti-TNF agent?
- Would combination therapy be appropriate?
In the algorithm, one can see that with controlled cancer beyond two years, the recommendation is to use a step-up approach.(23) Given that the patient is already on a biologic, one might consider a different biologic (e.g., back to anti-TNF, as she has previously done well on adalimumab).
In the specific context of breast cancer, there are data from three retrospective cohorts including women with rheumatoid arthritis or IBD who underwent surgery for primary breast cancer.(24) Risk of breast cancer recurrence was not found to be significantly elevated for methotrexate (HR 1.07, 95% CI 0.67–1.69), anti-TNF (HR 1.13, 95% CI 0.65–1.97) or thiopurines (HR 2.10, 95% CI 0.65–1.97).
In Sarah’s case, adalimumab was restarted, and her adalimumab drug level was checked post-load at the time of first maintenance, with no evidence of anti-drug antibodies detected. The seton was left in place, with reduced drainage after the addition of the adalimumab. The plan is to repeat colonoscopy six months after initiation of adalimumab while continuing standard follow up with her oncologist.
Risk Communication with Patients Regarding Malignancy
When communicating risk with patients, it is important to describe the risk-benefit ratio, including the risks of untreated inflammation over time. It is helpful to use absolute numbers and common denominators. The absolute risk of a disease can be explained as the risk of developing the disease over a time period, and can be expressed in different ways, e.g., 1 in 10 risk, 10% risk or 0.1 risk. Relative risk (RR) can be explained as a tool to compare the risk in two different groups of people, and is based on the absolute risk (e.g., RR of 10, 10-fold increased risk). When communicating risk to patients, it is best to avoid decimals, use common denominators, use visual aids to represent statistics graphically and, importantly, put risks into perspective with other disease and life risks.(25,26)
Prevention of Malignancy in IBD
Finally, prevention is possible for many forms of malignancy in IBD. Recommendations for primary and secondary preventive modalities (such as sunscreen use and screening tests) are important to prevent complications in the long term.
Conclusions
Patients with IBD are at increased risk for malignancy. As effective treatments have become available, GI malignancies have decreased while extraintestinal cancers have remained stable. In terms of IBD therapies, both thiopurines and anti-TNF agents have been associated with increased lymphoma risk and skin cancer risk. The risks of recurrence of cancer in IBD differ by initial type of malignancy. Although data are limited to date, what data we do have are reassuring with respect to risks of recurrence with immunosuppressive IBD therapies. When discussing risks and benefits with patients, clear communication is key, using absolute numbers and visual aids whenever possible. Finally, preventive strategies (e.g., regular sunscreen use) are important to implement for all IBD patients, as early as possible in the course of disease.
Clinical Case
Ann is a 63-year-old female with a long-standing history of ileocolonic and perianal Crohn’s disease (CD) with a history of multiple resections. She is an on-and-off smoker and has 1–2 drinks per week. She is on infliximab 5 mg/kg every four weeks and methotrexate (MTX) 12.5 mg weekly and is in clinical remission.
She presents with weight loss, painful swallowing and cervical lymphadenopathy. She underwent ultrasound of a necrotic lesion and biopsies show poorly differentiated carcinoma. She was referred to ENT for quadroscopy. Biopsies of tonsils revealed bilateral infiltrating, non-keratinizing, moderately differentiated squamous carcinoma. She is awaiting surgery and oncology assessment.
Her investigations revealed:
- WBC: 6.6 x 109/L
- Hemoglobin: 109 g/L
- CRP: 2.4 mg/L
- Albumin: 28 g/L
- Fecal calprotectin (FCP): 156 mcg/g
Commentary
While an individual with IBD who receives a cancer diagnosis will almost certainly shift his or her primary focus to the cancer, the management of the IBD and its potential complications (e.g., colorectal cancer [CDC]) should still be a consideration.(27)
Although there are no clinical practice guidelines to inform this decision, if the patient is amenable to colonoscopy while waiting for her surgery and oncology assessment, this can be considered, to assess her endoscopic disease activity and monitor for CRC.
With respect to her IBD medications, consultation and collaboration with the oncology team is essential. Notably, achievement of IBD remission during cytotoxic cancer therapy is common, so cessation of the IBD medications may be considered.(27,28) Although there are limited data on impact of anti-TNF therapy in tonsil cancer, there have been reports of negative impact on outcomes of other cancers (including survival) with anti-TNF agents.(29–31) The European evidence-based consensus on IBD and malignancies (2015) recommends that “In general, thiopurines, calcineurin inhibitors, and anti-TNF agents should be stopped at least until cancer therapy is completed.”(32) It is unlikely that continuing the MTX would be harmful, given that the safety profile of MTX is well known in other disciplines (e.g., rheumatology) and is also used as a chemotherapeutic agent to treat head and neck cancers.(33)
Her tonsil cancer may be related to her IBD, but not likely to her IBD medications. The European consensus paper stated that while “the overall risk of extraintestinal cancer in patients with IBD is not increased relative to the general population”, “individual cancer sites shows that CD patients are more likely to develop cancers of the upper gastrointestinal tract, lung, urinary bladder, and non-melanoma skin cancers, and UC is associated with an increased risk of liver-biliary tract cancers and leukaemia.”(32)
Although cigarette smoking is the more significant risk factor for her tonsil cancer, there is some evidence that IBD itself may be a risk factor.(33) As mentioned above, MTX is unlikely to be implicated in the tonsil cancer.(33) Anti-TNF medications have also not been linked with oral cancers in any clinical or large real-world studies.(27, 31–35)
Case Evolution
After discussion with the patient, you decided to hold her MTX and infliximab while she undergoes treatment for her malignancy. She is afraid her disease will flare if she holds her CD medications for too long.
She underwent surgical resection for her malignancy. She was seen by the oncologist who recommended cisplatin chemotherapy and radiation. The patient declined chemotherapy but accepted radiotherapy.
Commentary
With respect to this type of surgery, there are no data available to guide decision-making for IBD monitoring and management. However, in general, evidence suggests no difference in post-surgical complication rates for individuals with CD continuing or holding their biologics and immunosuppressants for surgical procedures.(36)
Although there is evidence showing that cytotoxic chemotherapy can have a beneficial impact on IBD response and remission, there is no such potential benefit for IBD with radiation. As such, it is logical to consider her CD as entirely untreated while her anti-TNF and MTX are held. Notably, it has been shown that TNF-α acts as a radiosensitizer and enhances the cytotoxic effect of radiation.(37,38) Inhibition of this pathway may, therefore, be detrimental to the anti-cancer potency of the radiotherapy.(36) Holding the anti-TNF until the radiotherapy is complete would be prudent. The European consensus document recommends that “In general, thiopurines, calcineurin inhibitors, and anti-TNF agents should be stopped at least until cancer therapy is completed.”(32)
Case Evolution
She undergoes six weeks of radiotherapy. She had a percutaneous endoscopic gastrotomy (PEG) tube inserted to help with nutrition as she had difficulty swallowing post-operatively. You do fecal calprotectin testing every three months:
- January: 228 mcg/g
- April: 1286 mcg/g
Clinically she is doing okay, with two to three bowel movements daily and no significant abdominal pain. Her perianal disease is inactive. She has completed her radiotherapy. You decide to restart therapy, as the fecal calprotectin is rising.
Commentary
One of the questions the patient may have is the risk of cancer recurrence related to her IBD medications. Data to date are reassuring, albeit limited, in regard to the impact of various IBD therapies on recurrence.(20)
The European consensus paper stated that “In IBD patients with a history of cancer, the risk of developing new or recurrent cancer is increased 2-fold relative to that of IBD patients who have never had cancer, regardless of whether or not they receive immunosuppressants.”(32) The consensus paper also states that “Preliminary data on immune-mediated inflammatory diseases and IBD demonstrate no obvious excess risk of developing a second [new or recurrent] cancer while being treated with anti-TNF therapy” and “In patients with active IBD and a history of malignancy, 5-aminosalicylates, nutritional therapies, and local corticosteroids can be safely used. In more severe flares that do not respond to these treatments, the use of anti-TNF, methotrexate, short-term systemic corticosteroids, and/or surgery should be considered on a case-by-case basis.”(32)
If she had been on chemotherapy, the course of action would depend on her IBD disease activity. As previously mentioned, cytotoxic chemotherapy can be associated with improvements in IBD activity and remission.(27,28) If there is active IBD, however, one might consider a course of steroids, anti-TNF or vedolizumab.(27)
Case Evolution
She receives a standard three-dose induction regimen of infliximab adjusted to her new weight. You decide to use monotherapy and not restart the immunomodulator. Repeat fecal calprotectin in four months is 56 mcg/g. She continues to follow with oncology, ENT, and gastroenterology. She requires repeat dilations of her postradiotherapy esophageal stricture.
Commentary
This patient was doing well with anti-TNF + MTX therapy prior to her cancer diagnosis. At the time her fecal calprotectin began to increase, she was still undergoing radiation therapy—although this was complete by the time the decision to restart IBD therapy was made. If the decision was made earlier (i.e., during the course of radiation therapy), then a biologic with an alternate mechanism of action (i.e., vedolizumab) might be considered.
As mentioned previously, restarting the anti-TNF biologic is supported by consensus recommendations for a person with a history of cancer.(27,32) Experience with vedolizumab is much more limited relative to anti-TNF biologics.(27) Although its clinical trial experience and early real-world data seem to indicate it has a favorable safety profile with respect to malignancies, longer-term experience is desirable before definitive recommendations can be made.
References
-
van den Heuvel TR, Wintjens DS, Jeuring SF, et al. Inflammatory bowel disease, cancer and medication: Cancer risk in the Dutch population-based IBDSL cohort. Int J Cancer. 2016;139(6):1270–80.
-
Kappelman MD, Farkas DK, Long MD, et al. Risk of cancer in patients with inflammatory bowel diseases: a nationwide population-based cohort study with 30 years of follow-up evaluation. Clin Gastroenterol Hepatol. 2014;12:265–73.
-
Beaugerie L, Itzkowitz SH. Cancers complicating inflammatory bowel disease. N Engl J Med. 2015;372(15):1441–52.
-
Long MD, Martin CF, Pipkin CA, et al. Risk of melanoma and nonmelanoma skin cancer among patients with inflammatory bowel disease. Gastroenterology. 2012;143:390–99.
-
Colombel J- F, Sands BE, Rutgeerts P, et al. The safety of vedolizumab for ulcerative colitis and Crohn’s disease. Gut. 2017;66:839–51.
-
Panaccione R, Danese S, Sandborn WJ, et al. Ustekinumab is effective and safe for ulcerative colitis through 2 years of maintenance therapy. Aliment Pharmacol Ther. 2020;52(11-12):1658–75.
-
Muller M, Broséus J, Feugier P, et al. Characteristics Of Lymphoma In Patients With Inflammatory Bowel Disease: A Systematic Review. J Crohns Colitis. 2020;Sep 19 [Epub ahead of print].
-
Lemaitre M, Kirchgesner J, Rudnichi A, et al. Association Between Use of Thiopurines or Tumor Necrosis Factor Antagonists Alone or in Combination and Risk of Lymphoma in Patients With Inflammatory Bowel Disease. JAMA. 2017;318(17):1679–86.
-
Beaugerie L, Brousse N, Bouvier AM, et al. Lymphoproliferative disorders in patients receiving thiopurines for inflammatory bowel disease: a prospective observational cohort study. Lancet. 2009;374(9701):1617–25.
-
Kirchgesner J, Beaugerie L, Carrat F, et al. Impact on Life Expectancy of Withdrawing Thiopurines in Patients with Crohn’s Disease in Sustained Clinical Remission: A Lifetime Risk-Benefit Analysis. PLoS One. 2016;11(6):e0157191.
-
Thai A, Prindiville T. Hepatosplenic T-cell lymphoma and inflammatory bowel disease. J Crohns Colitis. 2010;4(5):511–22.
-
Kotlyar DS, Osterman MT, Diamond RH, et al. A systematic review of factors that contribute to hepatosplenic T-cell lymphoma in patients with inflammatory bowel disease. Clin Gastroenterol Hepatol. 2011;9(1):36–41.
-
Deepak P, Sifuentes H, Sherid M, et al. T-cell non-Hodgkin’s lymphomas reported to the FDA AERS with tumor necrosis factor-alpha (TNF-α) inhibitors: results of the REFURBISH study. Am J Gastroenterol. 2013;108(1):99–105.
-
Long MD, Herfarth HH, Pipkin CA, et al. Increased risk for non-melanoma skin cancer in patients with inflammatory bowel disease. Clin Gastroenterol Hepatol. 2010;8(3):268–74.
-
O’Donovan P, Perrett CM, Zhang X, et al. Azathioprine and UVA light generate mutagenic oxidative DNA damage. Science. 2005;309(5742):1871–4.
-
Long MD, Weaver K, Kappelman MD, et al. Photosensitivity to Ultraviolet Light in Patients with Inflammatory Bowel Disease Newly Initiating Immunosuppressive Therapy. Inflamm Bowel Dis. 2016;22(1):E2–3.
-
Srivastava B. Systemic therapy and the risk of non- melanoma skin cancer among patients in the Psoriasis Longitudinal Assessment and Registry. Presented at EADV 2017; Free Communication #FC02.04
-
Curtis JR, Lee EB, Martin G, et al. Analysis of non-melanoma skin cancer across the tofacitinib rheumatoid arthritis clinical programme. Clin Exp Rheumatol. 2017; 35(4):614–22.
-
Sands BE, Long MD, Baidoo L, et al. An Update on the Analysis of Non-Melanoma Skin Cancer in the Tofacitinib Ulcerative Colitis Program [abstract #671]. Am J Gastroenterol. 2018; 114(Supp):S395.
-
Shelton E, Laharie D, Scott FI, et al. Cancer Recurrence Following Immune-Suppressive Therapies in Patients With Immune-Mediated Diseases: A Systematic Review and Meta-analysis. Gastroenterology. 2016;151:97–109.
-
Beaugerie L, Carrat F, Colombel JF, et al. Risk of new or recurrent cancer under immunosuppressive therapy in patients with IBD and previous cancer. Gut. 2014;63(9):1416–23.
-
Vedamurthy A, Gangasani N, Ananthakrishnan AN. Vedolizumab or Tumor Necrosis Factor Antagonist Use and Risk of New or Recurrent Cancer in Patients With Inflammatory Bowel Disease With Prior Malignancy: A Retrospective Cohort Study. Clin Gastroenterol Hepatol. 2020;Oct 13[Epub ahead of print].
-
Bernheim O, Colombel JF, Ullman TA, et al. The management of immunosuppression in patients with inflammatory bowel disease and cancer. Gut. 2013;62(11):1523–8.
-
Mamtani R, Clark AS, Scott FI, et al. Association Between Breast Cancer Recurrence and Immunosuppression in Rheumatoid Arthritis and Inflammatory Bowel Disease: A Cohort Study. Arthritis Rheumatol. 2016;68(10):2403–11.
-
Fagerlin A, Ubel PA, Smith DM, et al. Making numbers matter: present and future research in risk communication. Am J Health Behav. 2007;31(Suppl.1):S47–56.
-
Peters E, Hibbard J, Slovic P, et al. Numeracy skill and the communication, comprehension, and use of risk-benefit information. Health Aff (Millwood). 2007;26(3):741–8.
-
Sebastian S, Neilaj S. Practical guidance for the management of inflammatory bowel disease in patients with cancer. Which treatment? Therap Adv Gastroenterol. 2019;12:1756284818817293.
-
Axelrad JE, Fowler SA, Friedman S, et al. Effects of cancer treatment on inflammatory bowel disease remission and reactivation. Clin Gastroenterol Hepatol. 2012;10:1021–27.
-
Raaschou P, Simard JF, Neovius M, et al. Does cancer that occurs during or after anti tumour necrosis factor therapy has a worse prognosis. Arthritis Rheum. 2011;63:1812–22.
-
Nissen LHC, Pierik M, Derikx LA, et al. Risk factors and clinical outcomes in patients with IBD with melanoma. Inflamm Bowel Dis. 2017;23:2018–26.
-
Raaschou P, Simard JF, Holmqvist M, et al. Rheumatoid arthritis, anti-tumour necrosis factor therapy, and risk of malignant melanoma: nationwide population based prospective cohort study from Sweden. BMJ. 2013;346:1939–47.
-
Annese V, Beaugerie L, Egan L, et al. ECCO. European Evidence-based Consensus: Inflammatory Bowel Disease and Malignancies. J Crohns Colitis. 2015;9(11):945–65.
-
Katsanos KH, Roda G, Brygo A, et al. Oral Cancer and Oral Precancerous Lesions in Inflammatory Bowel Diseases: A Systematic Review. J Crohns Colitis. 2015;9(11):1043–52.
-
Greuter T, Vavricka S, König AO, et al. Malignancies in Inflammatory Bowel Disease. Digestion. 2020;101 Suppl 1:136–45.
-
Waljee AK, Higgins PDR, Jensen CB, et al. Anti-tumour necrosis factor-α therapy and recurrent or new primary cancers in patients with inflammatory bowel disease, rheumatoid arthritis, or psoriasis and previous cancer in Denmark: a nationwide, population-based cohort study. Lancet Gastroenterol Hepatol. 2020;5(3):276–84.
-
Marchal L, D’Haens G, Van Assche G, et al. The risk of post-operative complications associated with infliximab therapy for Crohn’s disease: a controlled cohort study. Aliment Pharmacol Ther. 2004;19:749–54.
-
Hallahan DE, Beckett MA, Kufe D, et al. The interaction between recombinant human tumor necrosis factor and radiation in 13 human tumor cell lines. Int J Radiat Oncol Biol Phys. 1990;19:69–74.
-
Wu X, Wu MY, Jiang M, et al. TNF-α sensitizes chemotherapy and radiotherapy against breast cancer cells. Cancer Cell Int. 2017;17:13.
Editor-in-Chief
John K. Marshall, MD MSc FRCPC AGAF, Director, Division of Gastroenterology, Professor, Department of Medicine, McMaster University, Hamilton, ON
Contributing Author
Millie D. Long, MD MPH, Associate Professor of Medicine, Division of Gastroenterology and Hepatology; Director, Gastroenterology and Hepatology Fellowship Program, University of North Carolina, Chapel Hill, North Carolina USA
Mentoring in IBD Curriculum Steering Committee
Alain Bitton, MD FRCPC, McGill University, Montreal, QC
Anne M. Griffiths, MC FRCPC, University of Toronto, Toronto, ON
Karen I. Kroeker, MD MSc FRCPC, University of Alberta, Edmonton, AB
Cynthia Seow, MBBS (Hons) MSc FRACP, University of Calgary, Calgary, AB
Jennifer Stretton, ACNP MN BScN, St. Joseph’s Healthcare, Hamilton, ON
IBD Dialogue 2021·Volume 17 is made possible by unrestricted educational grants from…
![]()
![]()



![]()
Published by Catrile & Associates Ltd., 167 Floyd Avenue, Toronto, ON M4J 2H9
(c) Catrile & Associates Ltd., 2021. All rights reserved. None of the contents may be reproduced in any form without prior written permission from the publisher. The opinions expressed in this paper are those of the authors and do not necessarily reflect the opinions or recommendations of the sponsors, the grantor, or the publisher.