Bone Health & IBD
Bone Health & IBD
March 28, 2023
Prevalence of Osteoporosis and Fracture in IBD
The objectives of Dr. Ananthakrishnan’s presentation were to discuss the epidemiology of osteoporosis, and how to assess and manage bone health in IBD management. Estimates of the prevalence of osteoporosis in IBD vary depending on the population sampled (age, disease features) and mode of assessment (dual energy x-ray absorptiometry [DXA] vs. clinical assessment). A systematic review identified 12 studies that included 3,661 patients with IBD, and found a prevalence rate of 2–16%, and more specifically 7–15% for Crohn’s disease (CD), and 2–9% for ulcerative colitis (UC), compared to 3–10% for the general population.(1)
Similarly, a population-based cohort in Denmark of 513 patients with IBD (213 CD; 300 UC) found a prevalence of osteoporosis of 14% in IBD patients, which was significantly increased vs. controls. Furthermore, the results showed that it remained significantly more prevalent even in patients <50 years of age.(2) With respect to the involvement of specific sites, a systematic review of 16 studies examining bone mineral density (BMD) in patients with IBD found that patients with IBD have lower BMD at the femoral neck as well as the lumbar spine, suggesting these are not site-specific effects.(3)
When thinking about the implications of reduced bone health in IBD, it is important to consider fracture risk. To this end, a Korean study based on insurance claims of 18,228 patients newly diagnosed with IBD showed a significantly higher risk of vertebral and hip fracture in CD and UC vs. age- and sex-matched controls at 2-, 5-, and 7-years post-diagnosis, an increase that was amplified in those taking steroids.(4)
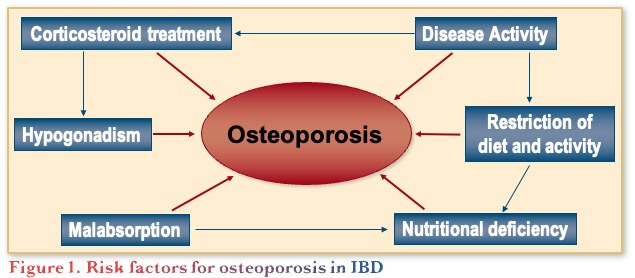
The general risk factors for osteoporosis are reasonably well understood and include female gender, older age, family history of osteoporosis, low body mass index, shorter height, ethnicity (Caucasian and Asian), smoking, and excess alcohol intake, noting that these can have a cumulative impact. In addition, risk factors related to IBD include disease activity, restriction of diet, steroid treatment, etc. (Figure 1).(1)
Steroid-induced osteoporosis impacts bone health through different mechanisms following short (acute) and long term (chronic) use. Increased fractures may be noted in as many as 30–50% of steroid users,(5,6) with the increase seen with prednisone doses as low as 2.5–7.5 mg/day or within 30 days of use. The incidence of fractures rises with increasing dose, duration, and age.(5,7)
Assessment of Bone Health in IBD
It is recommended that patients with IBD be screened based on established guidelines for the general population, which include screening women >65 years of age and men >70 years of age, adults with fracture >50 years of age, and any adult with fracture not caused by trauma. Factors specifically relevant for patients with IBD include the use of prednisone-equivalent >7.5 mg/day for >3 months, noting there is not an absolute cut off with regards to steroid impact on bone health.(8)
To quantify fracture risk, the Fracture Risk Assessment (FRAX) Tool was developed to calculate the 10-year probability of hip fracture and major osteoporosis-related fracture using a web-based system (https://osteoporosis.ca/frax/). High risk is defined as ≥20% for major fracture or ≥3% for hip fracture.(9) DXA is the most widely used method for assessing bone health using measurements from the lumbar spine, proximal femur, and femur neck.(10)
Management of Osteoporosis in IBD
Non-Pharmacologic Management of Osteoporosis
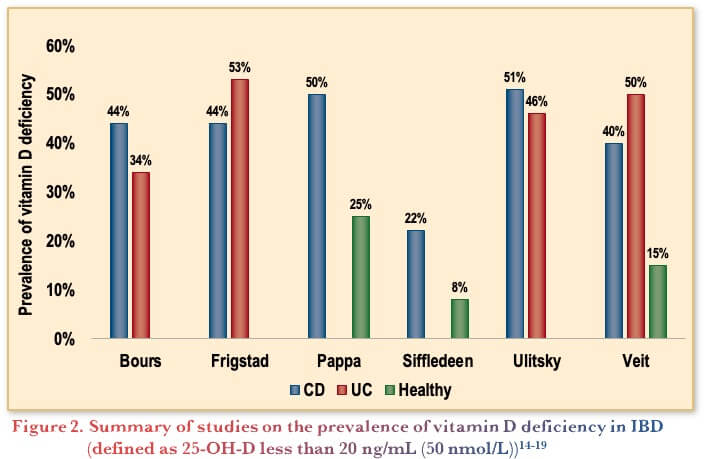
There is a large role for non-pharmacologic interventions in the management of osteoporosis. Specifically, it is recommended to maintain sufficient calcium and vitamin D intake with a target serum vitamin D level of 30–50 ng/mL. Thus, a daily supplementation of >400–800 IU, as well as daily calcium intake of 1000–1200 mg, is recommended. Calcium uptake preferably through diet as calcium supplementation in non-institutionalized adults is not supported by evidence.(11) With respect to Vitamin D, the targets are based on bone health, thus are not meant to assess any potential immunological effects. In terms of the role of vitamin D in IBD, deficiency is common in people with IBD (Figure 2). Furthermore, in observational studies vitamin D deficiency is associated with more severe disease in IBD, however it is not established if this is a cause or a consequence of the disease.(12,13)
In terms of vitamin D treatment in IBD, initial studies showed reduced rates of relapse in patients treated with vitamin D.(20) However, a more recent meta-analysis of 17 trials with 1,127 patients with IBD showed that oral vitamin D supplementation increased serum vitamin D levels and reduced C-reactive protein levels but did not decrease erythrocyte sedimentation rate (ESR), disease activity, or rates of relapse.(21)
Calcium and vitamin D supplementation is important for improving BMD; however, they can take years to have an impact. Specifically, a study of 154 patients with CD with decreased BMD randomized half the patient to etidronate (400 mg orally) treatment for 14 days, while all patients received daily calcium 500 mg and vitamin D 400 IU x 76 days. This cycle was repeated 8 times over 2 years. The results showed that the increase in BMD was similar in both groups showing no additional therapeutic benefit of etidronate.(20) Another study showed the benefits of calcium (500–1000 mg) and vitamin D (800 IU) supplementation of 205 CD patients with known risk factors for low BMD beyond CD. Specifically, looking at 84 patients who underwent a second BMD within a median of 4 years, an increase in mean BMD in lumbar spine and total hip was observed in those receiving supplementation.(22)
Other non-pharmacological interventions for modifiable risk factors include reducing caffeine (<4 cups of coffee / day), smoking cessation, reducing alcohol consumption (<2 drinks / day), fall risk assessment, as well as physical therapy and exercise.(11)
Studies have specifically investigated the impact of exercise on BMD in IBD. For example, a study of 117 patients with CD randomized to low-impact exercise or control for 12 months found that in the overall cohort there was no significant difference in BMD between the exercise group and controls. However, when considering only the fully compliant cohort, exercise was significantly associated with an increase in BMD.(23) Another small, randomized-controlled study of 47 patients with CD assigned to exercise (regular impact and resistance training for 6 months) or control found that the BMD values were superior in the exercise group with statistical significance achieved at the lumbar spine site. The exercise group also had superior values for muscle function outcomes such as grip strength and the chair stand test, suggesting a benefit for reducing future fracture risk and disability, important considerations for keeping patients functioning well.(24)
Pharmacologic Treatment of Osteoporosis
Several specific therapeutic options are currently available for the treatment of osteoporosis. An algorithm was developed by The Endocrine Society to guide clinicians in the selection of the most appropriate therapeutic choices when discussing with the patient (Figure 3). The two main treatment options are anti-resorptive agents (e.g., bisphosphonates, denosumab), and agents that promote bone formation (e.g., teriparatide).(25)

With respect to bisphosphonate use in IBD, a meta-analysis of 13 RCTs (482 bisphosphonates, 441 control) showed that bisphosphonate treatment in IBD patients reduced BMD loss at the lumbar spine and decreased fracture risk, with no increase in adverse effects.(26)
In addition, to prevent steroid-induced osteoporosis, it is recommended to use the lowest dose and shortest duration of steroids, and to choose steroid-sparing regimens when able. Furthermore, topical therapy is preferred over enteral or parenteral glucocorticoids.(27)
Conclusions
To summarize, suboptimal bone health can have profound consequences on patients with IBD. Therefore, gastroenterologists should routinely incorporate the assessment of bone health in their management of patients with IBD, as improving bone health helps to optimize functional capacity.
Clinical Case
- You receive a letter from a General Practitioner asking you to order a bone mineral density (BMD) test for a shared patient as in your province
- BMD testing can only be ordered for patients under the age of 50 by certain specialist providers
Commentary
- In terms of what to do next, most gastroenterologists would review the patient’s chart to see if this specific patient warrants a BMD test
Case Evolution
- You decide to review his chart for risk factors for osteoporosis
- Patient is 36-year-old Caucasian male with history of ileocolonic and perianal Crohn’s disease
- Diagnosed at age 20
- He received 1 course of prednisone (standard taper) at presentation
- Continued on azathioprine and infliximab for maintenance
- After 1 year, azathioprine was discontinued
- He had a flare of disease 3 years later, at which point he:
- Received a course of budesonide
- Dose interval of infliximab changed to every 4 weeks
- Patient currently in clinical, biochemical and endoscopic remission
- Also diagnosed with primary sclerosing cholangitis (PSC) at age 22
- Only other medication is pantoprazole, which he takes for GERD
- Physically active with a body mass index of 22.5 kg/m2
- Former smoker
- Drinks 8–10 drinks per week
- Vitamin D level 3 months ago: 48 nmol/L
- Takes 2000 IU Vitamin D most days
- Fractured his tibia six months ago while skiing, requiring surgery
- You decide to order a BMD test
Commentary
- In terms of the optimal vitamin D level in patients with IBD, most participating gastroenterologists felt it was >75 or >100 nmol/L
- In terms of how often to monitor vitamin D, participants would monitor it every 3 months after starting treatment and then every 12 months
- Furthermore, it was noted that adherence is an issue with vitamin D supplementation, so when speaking with patients it is important to explain the overall potential benefits of supplementation
- Continued testing of vitamin D is of value but there is a need to be cognizant of the context and interpret the results accordingly, as its potential role in improving IBD is not yet clear, but given it is very benign and associated with other potential benefits beyond bone health, vitamin D levels should be optimized
Case Evolution
- You receive the BMD test results, and the T-scores indicate ‘low bone density’
- Spine 1.37
- Hip 1.5
Commentary
- Besides addressing lifestyle factors and adding calcium and vitamin D supplementation, most gastroenterologists will now refer to an osteoporologist, as most are not comfortable treating osteoporosis
- For those gastroenterologists comfortable prescribing bisphosphonates, they focus on patients that are chronic steroid users and post-menopausal women
- Another advantage of referral is that it may improve access to additional treatments
Case Evolution
- Patient is lactose intolerant
- Takes Vitamin D (most days) but no calcium supplementation
- Consumes 8 cups of black coffee daily
- Former smoker
- Drinks 8–10 drinks per week
- Physically active (skiing weekly in winter and biking twice a week in summer)
- Testosterone and PTH levels are normal
- You recommend calcium and Vitamin D supplementation
Commentary
- Most gastroenterologists recheck bone density 2–3 years after initiating supplementation, but some would check every 6–12 months in cases like this
- Ideally gastroenterologists collaborate with specialists, but given many complications related to bone health are preventable, gastroenterologists serve as front-line providers in a position to initiate prevention strategies to optimize the health of their patients
Case Evolution
- You re-check bone density after 2 years
- Scores remain in the ‘low bone density’ range
References
-
Kärnsund S, Lo B, Bendtsen F, et al. Systematic review of the prevalence and development of osteoporosis or low bone mineral density and its risk factors in patients with inflammatory bowel disease. World J Gastroenterol. 2020;26(35):5362–74.
-
Lo B, Holm J, Vester-Andersen-MK, et al. Incidence, risk Factors and evaluation of osteoporosis in patients with inflammatory bowel disease: A Danish population-based inception cohort with 10 years of follow-up. J Crohns Colitis 2020;14(7):904–14.
-
Szafors P, Che H, Barnetche T, et al. Risk of fracture and low bone mineral density in adults with inflammatory bowel diseases. A systematic literature review with meta-analysis. Osteoporos Int. 2018;29(11):2389–97.
-
Ahn HJ, Kim Y-J, Lee H-S, et al. High risk of fractures within 7 years of diagnosis in Asian patients with inflammatory bowel diseases. Clin Gastroenterol Hepatol. 2022;20(5):e1022–39.
-
Compston J. Management of glucocorticoid-induced osteoporosis. Nat Rev Rheumatol 2010;6:82–8.
-
Waljee AK, Rogers MAM, Lin P, et al. Short term use of oral corticosteroids and related harms among adults in the United States: population based cohort study. 2017;357:j1415.
-
Ilias I, Milionis C & Zoumakis E. An Overview of Glucocorticoid-Induced Osteoporosis. In: Endotext [Internet]. Feingold KR, Anawalt B, Blackman MR, et al., editors. South Dartmouth (MA): MDText.com, Inc.; Last update: March 19, 2022.
-
Farraye FA, Melmed GY, Lichtenstein GR, et al. ACG Clinical Guideline: Preventive care in inflammatory bowel disease. Am J Gastroenterol. 2017;112(2):241–58.
-
FRAX ®Fracture Risk Assessment Tool. Available at: https://www.sheffield.ac.uk/FRAX/tool.aspx?country=19
-
The international Society for Clinical Densitometry. Adult positions. Available at: https://iscd.org/learn/official-positions/adult-positions/. Accessed: January 2023.
-
Coronado-Zarco R, Olascoaga-Gómez de Léon A, García-Lara A. Nonpharmacological interventions for osteoporosis treatment: Systematic review of clinical practice guidelines. Osteoporos Sarcopenia. 2019;5(3):69–77.
-
Li J, Chen N, Wang D et al. Efficacy of vitamin D in treatment of inflammatory bowel disease: A meta-analysis. Medicine (Baltimore). 2018;97(46):e12662.
-
Guo Y, Zhang T, Wang Y, et al. Effects of oral vitamin D supplementation on inflammatory bowel disease: a systematic review and meta-analysis. Food Funct. 2021;12(17):7588–606.
-
Bours PHA, Wielders JPM, Vermeijden JR, et al. Seasonal variation of serum 25-hydroxyvitamin D levels in adult patients with inflammatory bowel disease. Osteopor Int. 2011;22:2857-67.
-
Frigstad SV, Høvik M, Jahnson J, et al. Vitamin D deficiency in inflammatory bowel disease: prevalence and predictors in a Norwegian outpatient population. Scand J Gastroenterol. 2017;52(1):100–6.
-
Pappa HM, Gordon CM, Saslowsky TM, et al. Vitamin D status in children and young adults with inflammatory bowel disease. 2006;118(5):1950–61.
-
Siffledeen JS, Fedorak RN, Siminoski K, et al. Randomized trial of etidronate plus calcium and vitamin D for treatment of low bone mineral density in Crohn’s disease. Clin Gastroenterol Hepatol. 2005;3(2):122–32.
-
Ulitsky A, Ananthakrisnan AN, Naik A, et al. Vitamin D deficiency in patients with inflammatory bowel disease: association with disease activity and quality of life. JPEN J Parenter Enteral Nutr. 2011;35(3):308–16.
-
Veit LE, Maranda L, Fong J, Nwosu BU. The vitamin D status in inflammatory bowel disease. PLOS One. 2014; 9(7): e101583.
-
Ananthakrishnan AN. Environment risk factors for inflammatory bowel disease. Gastroenterol Hepatol (NY). 2013;9(6):367–74.
-
Mouli VP, Ananthakrishnan AN. Review article: Vitamin D and inflammatory bowel disease. Aliment Pharmacol Ther. 2014;39(2):125–36.
-
Robinson RJ, Krzywicki T, Almond L, et al. Effect of a low-impact exercise program on bone mineral density in Crohn’s disease: a randomized controlled trial. 1998;115(1):36–41.
-
Jones K, Baker K, Speight R, et al. Combined impact and resistance training in adults with stable Crohn’s disease. Aliment Pharmacol Ther. 2020;52(6):964–75.
-
Bakker SF, Dik VK, Birgit IW, et al. Increase in bone mineral density in strictly treated Crohn’s disease patients with concomitant calcium and vitamin D supplementation. J Crohns Colitis. 2013;7(5):377–84.
-
Shoback D, Rosen CJ, Black DM, et al. Pharmacological management of osteoporosis in postmenopausal women: An Endocrine Society Guideline Update. J Clin Endocrinol Metab. 2020;105(3):587–94.
-
Yao L, Wang H, Dong W, et al. Efficacy and safety of bisphosphonates in management of low bone density in inflammatory bowel disease: A meta-analysis. Medicine (Baltimore). 2017;96(3):e5861.
-
Ali T, Lam D, Bronze MS, et al. Osteoporosis in inflammatory bowel disease. Am J Med. 2009;122(7):599–604.
Editor-in-Chief
John K. Marshall, MD MSc FRCPC AGAF, Director, Division of Gastroenterology, Professor, Department of Medicine, McMaster University, Hamilton, ON
Contributing Author
Ashwin Ananthakrishnan, MD MPH, Associate Professor of Medicine, Division of Gastroenterology, Massachusetts General Hospital & Harvard Medical School, Boston, MA, USA
Mentoring in IBD Curriculum Steering Committee
Alain Bitton, MD FRCPC, McGill University, Montreal, QC
Karen I. Kroeker, MD MSc FRCPC, University of Alberta, Edmonton, AB
Cynthia Seow, MBBS (Hons) MSc FRACP, University of Calgary, Calgary, AB
Jennifer Stretton, ACNP MN BScN, St. Joseph’s Healthcare, Hamilton, ON
Eytan Wine, MD PhD FRCPC, University of Alberta, Edmonton, AB
IBD Dialogue 2023·Volume 19 is made possible by unrestricted educational grants from…
![]() a
a
![]() a
a
![]()

![]()

![]()
![]()
![]()
Published by Catrile & Associates Ltd., 167 Floyd Avenue, East York, ON M4J 2H9
(c) Catrile & Associates Ltd., 2023. All rights reserved. None of the contents may be reproduced in any form without prior written permission from the publisher. The opinions expressed in this paper are those of the authors and do not necessarily reflect the opinions or recommendations of the sponsors, the grantor, or the publisher.