Advanced Therapy in IBD: Mix & Match?
Advanced Therapy in IBD: Mix & Match?
January 25, 2022
Introduction: Why Do We Need Combination Therapy in IBD?
The objective of this presentation was to discuss sequencing of therapies incorporating new molecules and new strategies in IBD with emphasis on combination biologics. The rationale for dual biologic therapy is that multiple pathways drive inflammatory process and that remission rates for currently available biologics remain limited when used as single agents. Furthermore, mechanistic failure can lead to secondary loss of response with single biologic agents, biologics used second- or third-line tend to be less effective, and agents effective for luminal disease may not be as effective for extraintestinal manifestations or other concomitant immune-mediated inflammatory diseases (IMIDs). This is particularly relevant given the burden of IBD often goes beyond the gut, and studies have shown that IBD patients have a 7.5 times higher risk of developing another IMID compared with non-IBD patients.(1)
Theoretical advantages of combined therapy include greater efficacy, prevention of immunogenicity, and increased drug concentrations. Potential disadvantages of combined therapy include increased adverse effects, unknown safety risks, the complexity and cost of the regimen, and an increased need for patient monitoring.
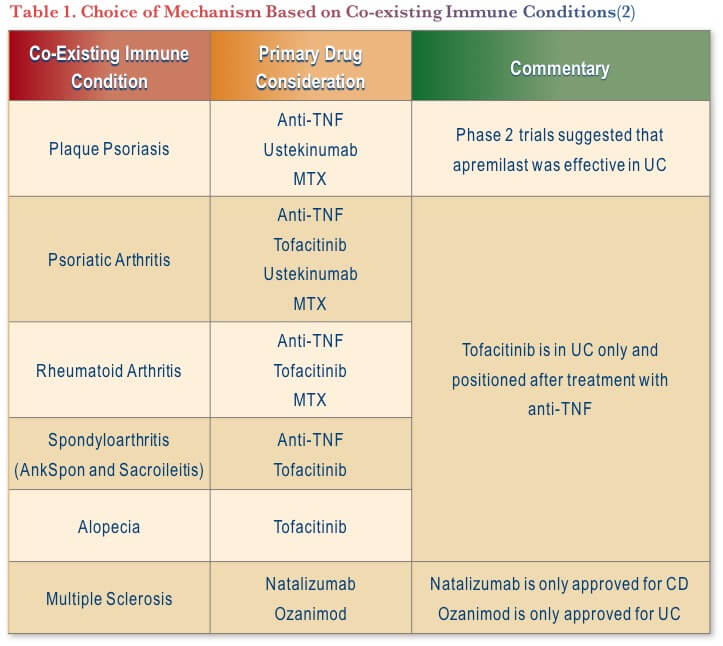
Clinical scenarios where combination strategies may be appropriate include refractory IBD or well-controlled IBD with an uncontrolled concomitant IMID. As the different mechanistic pathways underlying immune-modulated diseases are becoming better understood, there has been a shift towards a biology- and system-mediated approach to treatment selection, which may aid in selection of therapies with a common mechanism to one or more conditions. For example, when treating ulcerative colitis (UC) and ankylosing spondylitis (AS), an anti-TNF or tofacitinib may be the most appropriate choices (See Table 1).
Combination Therapy: Not a New Concept
The notion of combined therapy in IBD is not new. For example, in 2007 a trial of infliximab and natalizumab in combination was completed in patients with moderately to severely active Crohn’s Disease (CD). Results showed a non-significant efficacy trend in favor of combination therapy and found the combination well tolerated with no new safety signals, though the follow-up period was short.(3)
In addition, combination therapy with thiopurines is well established and data from the SONIC trial showed that the use of infliximab plus thiopurine in CD led to significantly more patients achieving steroid-free remission at week 26 than either therapy alone.(4) Further post hoc analysis investigating the exposure-response relationships determined that the benefit of combination therapy may be due to azathioprine’s influence on the pharmacokinetics of infliximab, in addition to an additive effect and reducing immunogenicity.(5)
In addition to efficacy, safety is a common concern associated with combination therapy. This was investigated within the TREAT Registry, which revealed no increased risk of infection associated with combination therapy. Risks of infection attributed to therapy may be offset by reduced susceptibility to infection with better disease control. (6)
Combination Therapy in Other Diseases
There are data on combination therapy from the rheumatology experience that may be of relevance to IBD. For example, a randomized-controlled trial (RCT) investigated the use of etanercept plus anakinra combination in patients with active rheumatoid arthritis (RA) despite methotrexate treatment. Results showed that the combination therapy for 6 months provided no additional treatment benefit nor immunogenicity. However, more serious infection, neutropenia, and injection site reactions occurred in the combination group leading the authors to recommend against the use of this combination in RA.(7)
Similar results were seen with an RCT of etanercept and abatacept in RA, showing no additional treatment benefits of combination therapy after 12 months but more serious adverse events (SAEs) and serious infections (SIs), again leading the authors to recommend against the use of this combination in RA.(8) Similar results were seen in another RCT that looked at anti-TNF/methotrexate combined with rituximab in RA.(9)
Lastly, a study on ABT-122, a bispecific variable domain immunoglobulin targeting TNF and interleukin (IL)-17A, in patients with RA with inadequate response to methotrexate (n=22) showed no meaningful efficacy benefit and no new safety signals up to 12 weeks over adalimumab alone.(10) Given the safety questions arising from these studies, a meta-analysis focusing on the safety of combination disease-modifying anti-rheumatic drugs (DMARDS) in RA concluded that there is no added benefit, while there is an increased risk of SAEs during the first twelve months of combination treatment.(11)
Combination Therapy in IBD
In IBD, data on combination therapy thus far are mainly from retrospective cohort studies or case reports. A recent review found that in all studies to date, combination therapy had positive outcomes, with only one study reporting an increased risk of infection.(12)
Specifically, a retrospective cohort study investigated the use of combination biologic or small molecule therapy in 50 patients with either IBD in remission and continued joint or skin inflammation or joint or skin in remission, but ongoing IBD activity. The study included a variety of combinations in UC and CD, most commonly with the base drug being vedolizumab. Results showed a significant increase in clinical and endoscopic remission rates with the introduction of combination therapy that was paralleled by improvement in biomarkers. Nothing atypical was observed in terms of safety.(13)
Another retrospective cohort study described 22 refractory patients with CD for whom a second biologic was added sequentially. In the majority of cases the baseline biologic was vedolizumab or ustekinumab and add-on was mainly anti-TNF. The results showed a significant improvement in endoscopic, clinical, and biomarker outcomes, and 38% of patients remained on dual therapy at 1 year. Surgery was needed in 33% of cases and nothing atypical was noted in terms of adverse events.(14)
Also relevant to this discussion is a study that looked at the safety of combination biologic and anti-rejection therapy in 20 IBD patients post liver transplantation. The case series combined with available literature concluded that there were no serious infections aside from C. difficile, which may be due to concurrent antibiotic use.(15)
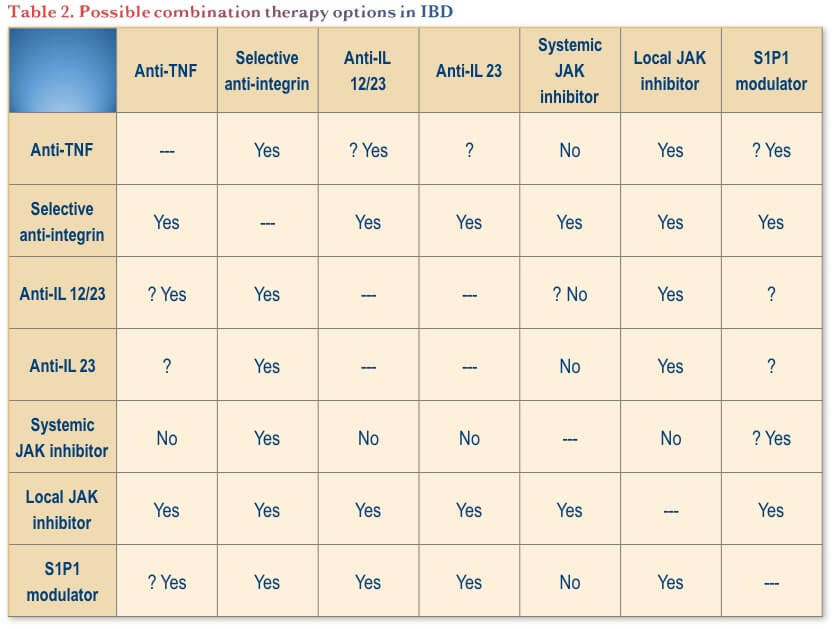
To summarize the data available to date on combination therapy in IBD, possible combinations to consider are summarized in Table 2.
Moving from Case Series to Clinical Trials in IBD
In terms of the future of combination therapy in IBD, there are some trials underway to help guide clinical practice:
- The EXPLORER open-label multicentre study is investigating triple combination therapy with an anti-integrin, an anti-TNF, and an immunomodulator (oral methotrexate) on endoscopic remission in participants with newly diagnosed CD stratified at higher risk for complications.(16)
- The VEGA study is a Phase 2a, randomized, double-blind, placebo-controlled, active-comparator-controlled, parallel-group, proof-of-concept, multicentre study evaluating the safety and efficacy of combination therapy with guselkumab and golimumab in patients with moderately to severely active UC.(17)
- The Duet UC and Duet CD studies are two Phase 2b studies investigating the impact of guselkumab combined with golimumab at induction vs. either alone over 48 weeks.(18,19)
Conclusions
To summarize, case series of combination therapy in IBD are generally positive, but our understanding of safety outcomes is limited by short follow-up durations. Furthermore, it can be debated whether observational studies from rheumatology that show no impact on efficacy and compromised safety can be extrapolated to IBD.
When facing patients with IBD that are refractory to treatments, it is important to review their medical records in detail to understand whether reported prior biological failures were indeed true failures and to characterize the nature of the failures. Some therapies can be re-introduced, combination therapies with different immunomodulators can be tried, trial eligibility can be assessed, and surgery can be considered.
Failing these steps, combination biologic/small molecule therapy could be carefully considered with clear counselling regarding off-label use and unknown safety concerns. In terms of risk, it is important to weigh against the risk of untreated disease (recurrent surgery, total parenteral nutrition, etc.). Furthermore, a defined timeframe (e.g., 6 months) should be agreed upon for re-assessment. Data thus far best support the use of vedolizumab or ustekinumab as anchor biologic.
Clinical Case
Jacqueline is a 32-year-old female working as a paramedic with an eight-year history of ileocolonic CD. She initiated azathioprine soon after diagnosis, then transitioned to methotrexate. Adalimumab was commenced 5 years ago but concomitant methotrexate subsequently stopped at her request after 1 year of combination therapy. Her CD has been ‘controlled’ with 40 mg of adalimumab every 2 weeks as monotherapy for the last 4 years.
She reports increasing symptoms over the last 6 months, during which time she had the initial COVID vaccine, the second dose and most recently a booster dose. She currently has three semi-formed bowel movements (BMs) per day, abdominal cramps and feels fatigued.
Her investigations reveal:
- WBC: 8.0 x 109/L
- Hb: 98 g/L
- CRP: 7 mg/L
- Alb: 34 g/L
- Fecal calprotectin: 2671 mcg/g
- Stool C and S negative
- C. difficile negative
Commentary
With regard to COVID vaccination in patients with IBD(20):
- Evaluation of adverse events (AEs) in a longitudinal vaccine registry found that the frequency of AEs in individuals with IBD is similar to that in the general population.
- Of note, those receiving biologic therapy were less likely to report AEs than those not on biologic therapies (36% vs. 47% after dose 1, p=0.17; 54% vs. 82% after dose 2, p=0.013).
Management strategies in this patient include optimization of her current treatment or switching to another treatment:
- The CAG Clinical Practice Guidelines for the Management of Luminal CD recommend dose optimization to recapture complete remission in patients with CD who lose response to anti-TNF maintenance therapy (conditional recommendations, very low-quality evidence).(21)
- Considering the limited data and guidance, clinicians must consider the risks of optimization vs. switching when making treatment decisions. Specifically, there is a need to weigh the benefits of rapid response and remission, while avoiding the risk of burning through treatments.
- Also, there are potential benefits of optimizing the dose to avoid losing any gains achieved to date and moving on to a different treatment option that may not be successful or well tolerated.
- Overall, clinicians must weigh numerous factors when making this decision, including disease severity, previous treatment history, presence or risk of extraintestinal manifestations, etc.
- There is a lack of consensus on the role of therapeutic drug monitoring (TDM) as well as the target levels, but it can be a useful tool to help guide treatment decisions.
- The CAG Clinical Practice Guidelines for the Management of Luminal CD suggest that dose optimization for patients with CD who lose response to anti-TNF therapy be informed by TDM (conditional recommendation, very low-quality evidence).(21)
Case Evolution
You advise Jacqueline that the frequency of adverse effects to the COVID vaccine in individuals with IBD is similar to that reported in the general population, and of note, IBD patients on biologic therapy were less likely to experience an adverse effect. You decide to check an adalimumab level while on 40 mg every other week, which returns at 12.3 mcg/mL.
Bowel ultrasound reveals prominence of the terminal ileum and sigmoid. After discussion, you decide to dose escalate to 40 mg weekly for three months, then reevaluate. Unfortunately, her symptoms progress and she requests to change therapies, also mentioning new perianal discomfort.
Commentary
- The CAG Clinical Practice Guidelines for the Management of Luminal CD recommends imaging (EUS or MRI, based on availability and local expertise) be obtained in patients with CD and signs and/or symptoms of active fistulizing disease to delineate the anatomy of the fistula tract(s).(21)
In terms of therapeutic options to consider next for this patient:
- The 2021 AGA Technical Review on the Medical Management of Moderate to Severe Luminal and Perianal Fistulizing Crohn’s Diseases recommends that for patients with moderate to severely active CD with prior anti-TNF exposure, ustekinumab is probably more effective than no treatment (moderate certainty of evidence), and vedolizumab may be more effective than no treatment (low certainty of evidence) in inducing remission.(22)
- While there is a lack of head-to-head RCT studies, recent retrospective and prospective comparative studies have shown improved short and long-term effectiveness of ustekinumab vs. vedolizumab in patients who failed anti-TNF in terms of early and long-term effectiveness (corticosteroid-free clinical remission and/or biochemical remission).(23,24)
Case Evolution
Colonoscopy reveals moderate inflammation with occasional ulceration in the terminal ileum, the descending colon and the sigmoid without rectal involvement. Perianal examination is non-contributory, but digital rectal examination reveals moderate hemorrhoids, which you believe are contributing to her perianal discomfort.
Jacqueline declines any further anti-TNF therapy after reading reports of waning antibodies to COVID and is not reassured by her recent booster COVID vaccination. She requests a ‘gut-specific’ option that will not affect her ‘immune system’, so intravenous induction and subcutaneous maintenance doses of vedolizumab are provided.
At her 3 and 6-month follow-up appointments Jacqueline states she is far less fatigued and has an overall improved sense of well-being. She reports that she has been wearing a pad because of blood and “pus” leakage from her “hemorrhoids”. MRI demonstrates a small trans-sphincteric tract leading out to the gluteal skin corresponding to an updated perianal physical examination.
You increase the vedolizumab dosing to q4w for 6 months. There is further improvement in her bowel frequency and abdominal pain, and she achieves mucosal healing as evidenced by colonoscopy. You had hoped there may be some effect on her perianal disease, but the discomfort worsens, with the development of complex branching perianal fistulae.
Commentary
The 2021 AGA Technical Review on the Medical Management of Moderate to Severe Luminal and Perianal Fistulizing Crohn’s Diseases recommends the following for adults with symptomatic fistulizing CD:(22,25)
- Infliximab is probably effective for achieving and maintaining fistula closure (moderate certainty of evidence).
- The benefit of adalimumab and certolizumab pegol in achieving fistula closure is uncertain (very low certainty of evidence), while in patients with fistulizing CD in remission, adalimumab and certolizumab pegol may be effective for maintaining fistula closure (low certainty of evidence).
- The benefit of vedolizumab or ustekinumab in achieving and maintaining fistula closure is uncertain (low certainty of evidence).
- A systematic review and meta-analysis of data from 27 trials on the efficacy of medical therapies for fistulizing CD found moderate-quality evidence to support the efficacy of anti-TNFs (RR, 2.01; 95% CI, 1.36–2.97), particularly infliximab, ustekinumab (RR, 1.77; 95% CI, 0.93–3.37), and mesenchymal stem cell therapy (RR, 1.31; 95% CI, 0.98–1.73) for induction of fistula remission.(26)
- Low-quality evidence was found for the efficacy of vedolizumab and immunosuppressives and combination therapy with anti-TNFs and antibiotics vs. anti-TNF alone.
Case Evolution
You ponder whether to:
- Go back to an anti-TNF
- Add an anti-TNF to the existing vedolizumab
- Reintroduce an immunomodulator
- Switch to ustekinumab, or
- Wait for approval of the new IL-23 selective agents or JAK inhibitors
While you are scratching your head over these complex decisions, Jacqueline calls your office about a new skin rash on her neck, behind her ears, and on her lower limbs.
Commentary
- Currently, there are several therapeutic options with different mechanisms of action available for CD, including targeting TNF, interleukins 12 and 23, integrins and Janus Kinases.
- Newer biologics have several advantages including targeted inhibition of cytokines, safety, and low immunogenicity.
- Small molecules avoid immunogenicity, have a short half-life, and are convenient due to oral administration.
- There is a lack of guidance as to the sequencing of biologic therapy, which in practice is often dictated by reimbursement criteria.
- Recently, in an effort to raise the therapeutic ceiling for efficacy, the concept of combination biologics targeting different pathways is of interest for medically refractory disease. At this stage, the evidence for the safety and efficacy of this approach is limited, as discussed.
- Considering this patients patient’s previous response to adalimumab and the data supporting the use of anti-TNFs in perianal disease, adding adalimumab or infliximab back in might be considered.
- Thankfully, controlled clinical trials are now underway to explore the efficacy and safety of combination biologics in IBD.
References
-
Conway G, Velonias G, Andrews E, et al. The impact of co-existing immune-mediated diseases on phenotype and outcomes in inflammatory bowel diseases. Aliment Pharmacol Ther. 2017;45(6):814–23.
-
Schett G, McInnes IB, Neurath MF. Reframing immune-mediated inflammatory diseases through signature cytokine hubs. N Engl J Med. 2021;385(7):628–39.
-
Sands BE, Kozarek R, Spainhour J, et al. Safety and tolerability of concurrent natalizumab treatment for patients with Crohn’s disease not in remission while receiving infliximab. Inflamm Bowel Dis. 2007;13(1):2–11.
-
Colombel JF, Sandborn WJ, Reinisch W, et al, Infliximab, azathioprine, or combination therapy for Crohn’s Disease. N Engl J Med. 2010;362:1383–95.
-
Colombel JF, Adedokun OJ, Gasink C, et al. Combination therapy with infliximab and azathioprine improves infliximab pharmacokinetic features and efficacy: A post hoc analysis. Clin Gastroenterol Hepatol. 2019;17(8):1525–32.e1.
-
Lichtenstein GR, Feagan BG, Cohen RD, et al. Serious infection and mortality in patients with Crohn’s disease: More than 5 years of follow-up in the TREAT registry. Am J Gastroenterol. 2012;107(9):1407–22.
-
Genovese MC, Cohen S, Moreland L, et al. Combination therapy with etanercept and anakinra in the treatment of patients with rheumatoid arthritis who have been treated unsuccessfully with methotrexate. Arthritis Rheum. 2004;50(5):1412–19.
-
Weinblatt M, Schiff M, Goldman A, et al. Selective costimulation modulation using abatacept in patients with active rheumatoid arthritis while receiving etanercept: a randomised clinical trial. Ann Rheum Dis. 2007;66(2):228–34.
-
Greenwald MW, Shergy WJ, Kaine JL, et al. Evaluation of the safety of rituximab in combination with a tumor necrosis factor inhibitor and methotrexate in patients with active rheumatoid arthritis: Results from a randomized controlled trial. Arthritis Rheum. 2011;63(3):622–32.
-
Genovese M, Weinblatt ME, Aelion JA, et al. ABT-122, a bispecific dual variable domain immunoglobulin targeting tumor necrosis factor and interleukin-17A, in patients with rheumatoid arthritis with an inadequate response to methotrexate: A randomized, double-blind study. Arthritis Rheumatol. 2018;70(11):1710–20.
-
Boleto G, Kanagaratnam L, Dramé M, et al. Safety of combination therapy with two bDMARDs in patients with rheumatoid arthritis: A systematic review and meta-analysis. Sem Arthritis Rheum. 2019;49(1):35–42.
-
Gold SL, Steinlauf AF. Efficacy and safety of dual biologic therapy in patients with inflammatory bowel disease: A review of the literature. Gastroenterol Hepatol, 2021;17(9):406–14.
-
Glassner K, Oglat A, Duran A, et al. The use of combination biological or small molecule therapy in inflammatory bowel disease: A retrospective cohort study. J Dig Dis. 2020;21(5):26–71.
-
Yang E, Panaccione N, Whitmire N, et al. Efficacy and safety of simultaneous treatment with two biologic medications in refractory Crohn’s disease. Aliment Pharmacol Ther. 2020;51(11):1031–8.
-
Al Draiweesh S, Ma C, Alkhattabi M, et al. Safety of combination biologic and antirejection therapy post-liver transplantation in patients with inflammatory bowel disease. Inflamm Bowel Dis. 2020;26(6);949–59.
-
Triple Combination Therapy in High Risk Crohn’s Disease (CD) available at: ClinicalTrials.gov: NCT02764762.
-
A Study of Efficacy and Safety of Combination Therapy With Guselkumab and Golimumab in Participants With Moderately to Severely Active Ulcerative Colitis (VEGA). Available at: https://clinicaltrials.gov/ct2/show/NCT03662542.
-
A Study of Combination Therapy With Guselkumab and Golimumab in Participants With Moderately to Severely Active Ulcerative Colitis (DUET-UC). Available at: https://clinicaltrials.gov/ct2/show/NCT05242484
-
A Study of Combination Therapy With Guselkumab and Golimumab in Participants With Moderately to Severely Active Crohn’s Disease (DUET-CD). Available at: https://clinicaltrials.gov/ct2/show/NCT05242471
-
Botwin GJ, Li D, Figueiredo J, et al. Adverse events after SARS-CoV-2 mRNA vaccination among patients with inflammatory bowel disease. Am J Gastroenterol. 2021 Aug 1;116(8):1746–51.
-
Panaccione R, Steinhart AH, Bressler B, et al. Clinical Practice Guidelines. Canadian Association of Gastroenterology clinical practice guideline for the management of luminal Crohn’s disease. Clin Gastroenterol Hepatol. 2019;17(9):1680–1713.
-
Singh S, Proctor D, Scott FI, et al. AGA technical review on the medical management of moderate to severe luminal and perianal fistulizing Crohn’s Disease. 2021;160:2512–56.
-
Manlay L, Baschetti G, Pereira B, et al. Comparison of short- and long-term effectiveness between ustekinumab and vedolizumab in patients with Crohn’s disease refractory to anti-tumour necrosis factor therapy. Aliment Pharmacol Ther. 2021;53:1289–99.
-
Biermans VBC, van der Woude CJ, Dijkstra G, et al. Ustekinumab is associated with superior effectiveness outcomes compared to vedolizumab in Crohn’s disease patients with prior failure to anti-TNF treatment. Aliment Pharmacol Ther. 2020;52:123–34.
-
Steinhart AH, Panaccione R, Targownik L, et al. Clinical practice guideline for the medical management of perianal fistulizing Crohn’s disease: The Toronto Consensus. Inflamm Bowel Dis. 2019;25(1):1–13.
-
Lee MJ, Parker CE, Taylor SR, et al. Efficacy of medical therapies for fistulizing Crohn’s Disease: Systematic review and meta-analysis. Clin Gasteroenterol Hepatol. 2018;16:1879–92.
Editor-in-Chief
John K. Marshall, MD MSc FRCPC AGAF, Director, Division of Gastroenterology, Professor, Department of Medicine, McMaster University, Hamilton, ON
Contributing Author
Vipul Jairath, MBChB (hons) DPhil MRCP FRCPC, Professor of Medicine, Division of Gastroenterology, Western University, London Health Sciences Centre, London, ON
Mentoring in IBD Curriculum Steering Committee
Alain Bitton, MD FRCPC, McGill University, Montreal, QC
Anne M. Griffiths, MC FRCPC, University of Toronto, Toronto, ON
Karen I. Kroeker, MD MSc FRCPC, University of Alberta, Edmonton, AB
Cynthia Seow, MBBS (Hons) MSc FRACP, University of Calgary, Calgary, AB
Jennifer Stretton, ACNP MN BScN, St. Joseph’s Healthcare, Hamilton, ON
IBD Dialogue 2022·Volume 18 is made possible by unrestricted educational grants from…
![]()
![]()
![]()


![]()
![]()
![]()
Published by Catrile & Associates Ltd., 167 Floyd Avenue, North York, ON M4J 2H9
(c) Catrile & Associates Ltd., 2022. All rights reserved. None of the contents may be reproduced in any form without prior written permission from the publisher. The opinions expressed in this paper are those of the authors and do not necessarily reflect the opinions or recommendations of the sponsors, the grantor, or the publisher.